Department of Medicine, Division of General Internal Medicine, University of Minnesota Medical School, 420 Delaware St. SE MMC 741, Minneapolis, MN, 55455, USA.
Department of Pediatrics, University of Minnesota Medical School, Minneapolis, MN, 55455, USA.
BMC Health Serv Res. 2021 Apr 14;21(1):338. doi: 10.1186/s12913-021-06323-5.
Super-utilizers with 4 or more admissions per year frequently receive low-quality care and disproportionately contribute to healthcare costs. Inpatient care fragmentation (admission to multiple different hospitals) in this population has not been well described.
To determine the prevalence of super-utilizers who receive fragmented care across different hospitals and to describe associated risks, costs, and health outcomes.
We analyzed inpatient data from the Health Care Utilization Project's State Inpatient and Emergency Department database from 6 states from 2013. After identifying hospital super-utilizers, we stratified by the number of different hospitals visited in a 1-year period. We determined how patient demographics, costs, and outcomes varied by degree of fragmentation. We then examined how fragmentation would influence a hospital's ability to identify super-utilizers.
Adult patients with 4 or more inpatient stays in 1 year.
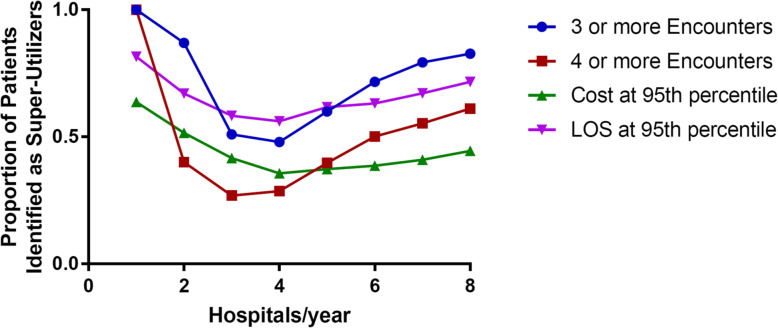
Patient demographics, cost, 1-year hospital reported mortality, and probability that a single hospital could correctly identify a patient as a super-utilizer.
Of the 167,515 hospital super-utilizers, 97,404 (58.1%) visited more than 1 hospital in a 1-year period. Fragmentation was more likely among younger, non-white, low-income, under-insured patients, in population-dense areas. Patients with fragmentation were more likely to be admitted for chronic disease management, psychiatric illness, and substance abuse. Inpatient fragmentation was associated with higher yearly costs and lower likelihood of being identified as a super-utilizer.
Inpatient care fragmentation is common among super-utilizers, disproportionately affects vulnerable populations. It is associated with high yearly costs and a decreased probability of correctly identifying super-utilizers.
每年住院 4 次或以上的超级使用者经常接受低质量的护理,并且不成比例地增加医疗保健费用。在该人群中,住院治疗碎片化(入住多家不同医院)尚未得到充分描述。
确定在不同医院接受碎片化护理的超级使用者的流行程度,并描述相关风险、成本和健康结果。
我们分析了来自 6 个州的健康护理利用项目州住院和急诊部数据库的住院数据。在确定了医院超级使用者之后,我们根据在 1 年内访问的不同医院数量进行分层。我们确定了患者人口统计学特征、成本和结果如何因碎片化程度而有所不同。然后,我们研究了碎片化将如何影响医院识别超级使用者的能力。
每年住院 4 次或以上的成年患者。
患者人口统计学特征、成本、1 年医院报告死亡率以及单个医院正确识别患者为超级使用者的概率。
在 167515 名医院超级使用者中,有 97404 名(58.1%)在 1 年内访问了多家医院。碎片化更可能发生在年轻、非白种人、低收入、保险不足的人群中,以及人口密集的地区。有碎片化的患者更可能因慢性病管理、精神疾病和药物滥用而住院。住院碎片化与更高的年度成本和更不可能被确认为超级使用者相关。
超级使用者的住院治疗碎片化很常见,不成比例地影响弱势群体。它与高额年度成本和正确识别超级使用者的可能性降低有关。