Department of Psychology, Rowan University, Glassboro, NJ, United States.
Device Evaluation, ECRI, Plymouth Meeting, PA, United States.
J Med Internet Res. 2021 Apr 15;23(4):e25657. doi: 10.2196/25657.
Obtaining accurate clinical information about recent acute care visits is extremely important for outpatient providers. However, documents used to communicate this information are often difficult to use. This puts patients at risk of adverse events. Elderly patients who are seen by more providers and have more care transitions are especially vulnerable.
This study aimed to (1) identify the information about elderly patients' recent acute care visits needed to coordinate their care, (2) use this information to assess discharge summaries, and (3) provide recommendations to help improve the quality of electronic health record (EHR)-generated discharge summaries, thereby increasing patient safety.
A literature review, clinician interviews, and a survey of outpatient providers were used to identify and categorize data needed to coordinate care for recently discharged elderly patients. Based upon those data, 2 guidelines for creating useful discharge summaries were created. The new guidelines, along with 17 previously developed medical documentation usability heuristics, were applied to assess 4 simulated elderly patient discharge summaries.
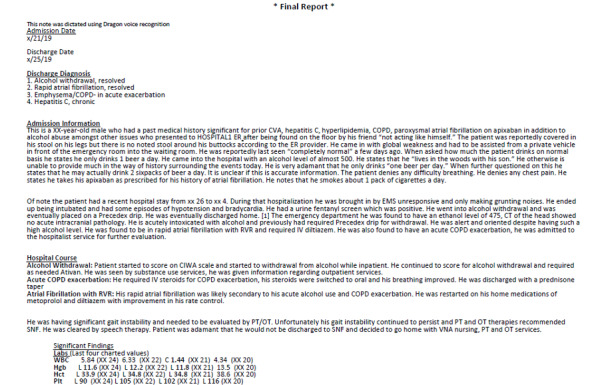
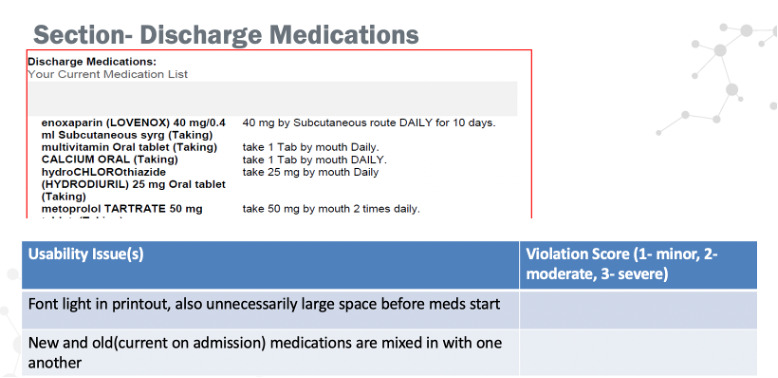
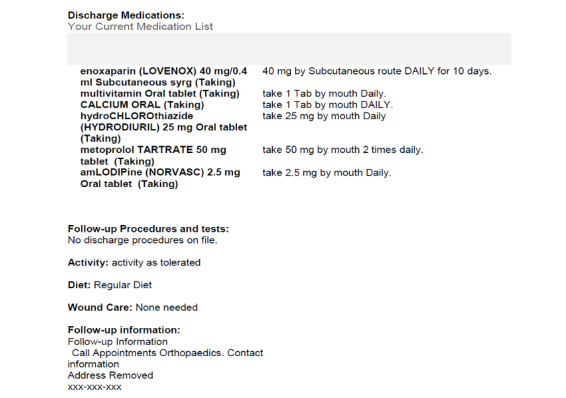
The initial research effort yielded a list of 29 items that should always be included in elderly patient discharge summaries and a list of 7 "helpful, but not always necessary" items. Evaluation of 4 deidentified elderly patient discharge summaries revealed that none of the documents contained all 36 necessary items; between 14 and 18 were missing. The documents each had several other issues, and they differed significantly in organization, layout, and formatting.
Variations in content and structure of discharge summaries in the United States make them unnecessarily difficult to use. Standardization would benefit both patients, by lowering the risk of care transition-related adverse events, and outpatient providers, by helping reduce frustration that can contribute to burnout. In the short term, acute care providers can help improve the quality of their discharge summaries by working with EHR vendors to follow recommendations based upon this study. Meanwhile, additional human factors work should determine the most effective way to organize and present information in discharge summaries, to facilitate effective standardization.
获取有关近期急性护理就诊的准确临床信息对门诊提供者极为重要。然而,用于传达这些信息的文档通常难以使用。这使患者面临不良事件的风险。接受过更多提供者就诊且有更多护理过渡的老年患者尤其脆弱。
本研究旨在:(1)确定协调老年患者护理所需的近期急性护理就诊信息;(2)使用这些信息评估出院小结;(3)提供建议,以帮助提高电子健康记录(EHR)生成的出院小结的质量,从而提高患者安全性。
通过文献回顾、临床医生访谈和对门诊提供者的调查,确定并分类了协调最近出院的老年患者护理所需的数据。基于这些数据,制定了 2 条用于创建有用的出院小结的指南。新指南与之前制定的 17 条医疗文档可用性启发式指南一起,应用于评估 4 个模拟老年患者出院小结。
最初的研究工作产生了一份清单,列出了 29 项在老年患者出院小结中应始终包含的项目,以及 7 项“有用但并非总是必要”的项目。对 4 份匿名老年患者出院小结的评估显示,没有一份文件包含所有 36 项必要项目;有 14 到 18 项缺失。这些文件都存在其他几个问题,在组织、布局和格式方面也存在显著差异。
美国出院小结的内容和结构存在差异,导致其使用不便。标准化将使患者受益,降低与护理过渡相关的不良事件风险,也将使门诊提供者受益,帮助减少可能导致倦怠的挫败感。在短期内,急性护理提供者可以通过与 EHR 供应商合作,根据本研究提出的建议来提高出院小结的质量。同时,还需要进行更多的人为因素研究,以确定在出院小结中组织和呈现信息的最有效方法,以促进有效的标准化。