Department of Trauma Surgery, Amsterdam UMC location VUmc, De Boelelaan 1117, 1081, HV, Amsterdam, The Netherlands.
Department of Anesthesiology, Amsterdam UMC location VUmc, De Boelelaan 1117, 1081, HV, Amsterdam, The Netherlands.
BMC Emerg Med. 2021 Apr 16;21(1):50. doi: 10.1186/s12873-021-00439-x.
For decades, Helicopter Emergency Medical Services (HEMS) contribute greatly to prehospital patient care by performing advanced medical interventions on-scene. Unnecessary dispatches, resulting in cancellations, cause these vital resources to be temporarily unavailable and generate additional costs. A previous study showed a cancellation rate of 43.5% in our trauma region. However, little recent data about cancellation rates and reasons exist, despite revision of dispatch protocols. This study examines the current cancellation rate in our trauma region over a six-year period. Additionally, cancellation reasons are evaluated per type of dispatch and initial incident report, upon which HEMS is dispatched.
This retrospective study analyzed the data of the Dutch HEMS Lifeliner 1 (North-West region of the Netherlands, covering a population of 5 million inhabitants), analyzing all subsequent cases between April 1st 2013 and April 1st 2019. Patient characteristics, type of dispatch (primary; based on dispatcher criteria versus secondary, as judged by the first ambulance team on site), initial incident report received by the EMS dispatch center, and information regarding day- or nighttime dispatches were collected. In case of cancellation, cancel rate and reason per type of dispatch and initial incident report were assessed.
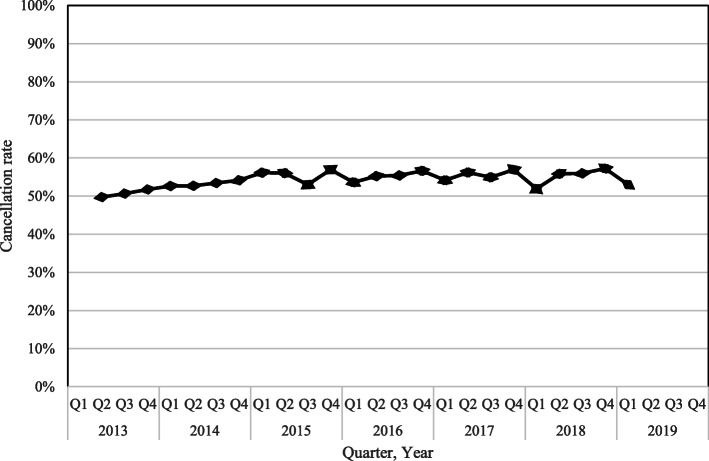
In total, 18,638 dispatches were included. HEMS was canceled in 54.5% (95% CI 53.8-55.3%) of cases. The majority of canceled dispatches (76.1%) were canceled because respiratory, hemodynamic, and neurologic parameters were stable. Dispatches simultaneously activated with EMS (primary dispatch) were canceled in 58.3%, compared to 15.1% when HEMS assistance was requested by EMS based on their findings on-scene (secondary dispatch). A cancellation rate of 54.6% was found in trauma related dispatches (n = 12,148), compared to 52.2% in non-trauma related dispatches (n = 5378). Higher cancellation rates exceeding 60% were observed in the less common dispatch categories, e.g., anaphylaxis (66.3%), unknown incident report (66.0%), assault with a blunt object (64.1%), obstetrics (62.8%), and submersion (61.9%).
HEMS cancellations are increased, compared to previous research in our region. Yet, the cancellations are acceptable as the effect on HEMS' unavailbility remains minimized. Focus should be on identifying the patient in need of HEMS care while maintaining overtriage rates low. Continuous evaluation of HEMS triage is important, and dispatch criteria should be adjusted if necessary.
几十年来,直升机紧急医疗服务(HEMS)通过在现场进行高级医疗干预,极大地促进了院前患者护理。不必要的派遣导致取消,使这些重要资源暂时无法使用并产生额外成本。先前的一项研究表明,在我们的创伤地区,取消率为 43.5%。然而,尽管派遣协议已经修订,但最近关于取消率和原因的数据很少。本研究在六年期间检查了我们的创伤地区的当前取消率。此外,还根据派遣的类型和最初的事件报告评估了取消原因,HEMS 根据该报告进行派遣。
这项回顾性研究分析了荷兰 HEMS Lifeliner 1(荷兰西北部地区,覆盖 500 万居民)的数据,分析了 2013 年 4 月 1 日至 2019 年 4 月 1 日期间的所有后续病例。收集了患者特征、派遣类型(主要,根据调度员标准与次要,由现场的第一急救队判断)、EMS 调度中心收到的初始事件报告以及日间或夜间派遣信息。在取消的情况下,按派遣类型和初始事件报告评估取消率和原因。
共纳入 18638 次派遣。HEMS 在 54.5%(95%CI 53.8-55.3%)的情况下被取消。取消的大多数派遣(76.1%)是因为呼吸、血流动力学和神经参数稳定。与 HEMS 协助根据他们在现场的发现同时激活的派遣(主要派遣)被取消了 58.3%,而当 HEMS 援助由 EMS 根据他们在现场的发现请求时,被取消的比例为 15.1%(次要派遣)。在与创伤相关的派遣(n=12148)中发现取消率为 54.6%,而在与创伤无关的派遣(n=5378)中发现取消率为 52.2%。在不太常见的派遣类别中观察到超过 60%的更高取消率,例如过敏反应(66.3%)、未知事件报告(66.0%)、钝器攻击(64.1%)、产科(62.8%)和淹没(61.9%)。
与我们地区以前的研究相比,HEMS 的取消有所增加。然而,由于对 HEMS 可用性的影响仍然最小化,取消是可以接受的。重点应该是在保持过筛率低的情况下确定需要 HEMS 护理的患者。持续评估 HEMS 分诊很重要,如果有必要,应调整派遣标准。