Department of Congenital Heart Disease, University Hospitals Bristol and Weston NHS Foundation Trust, Upper Maudlin Street, Bristol, BS2 8BJ, UK.
Pediatr Cardiol. 2021 Jun;42(5):1180-1189. doi: 10.1007/s00246-021-02599-w. Epub 2021 Apr 19.
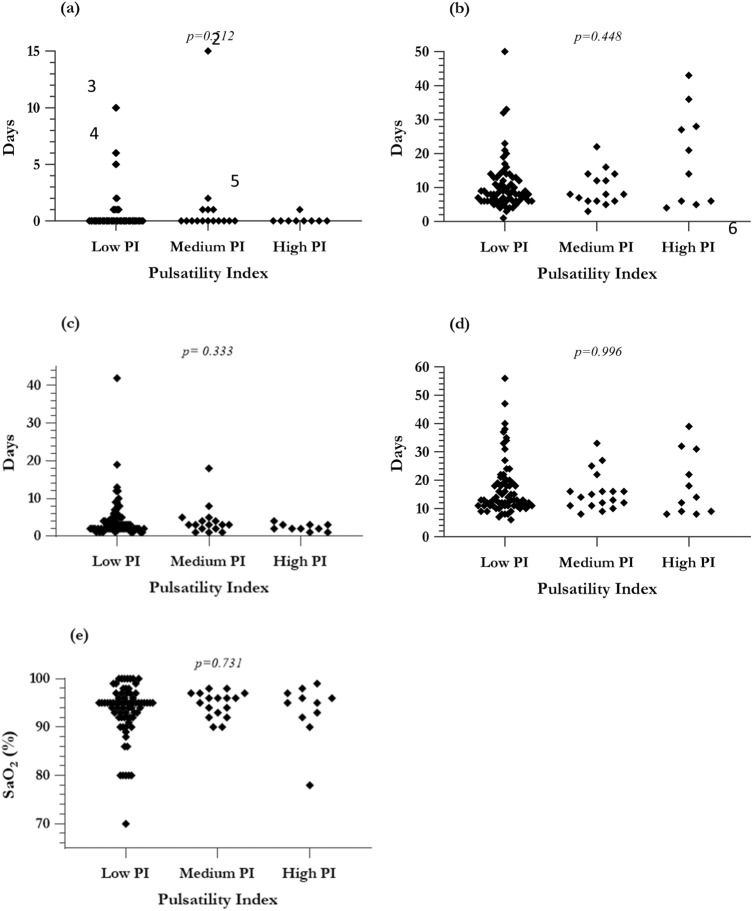
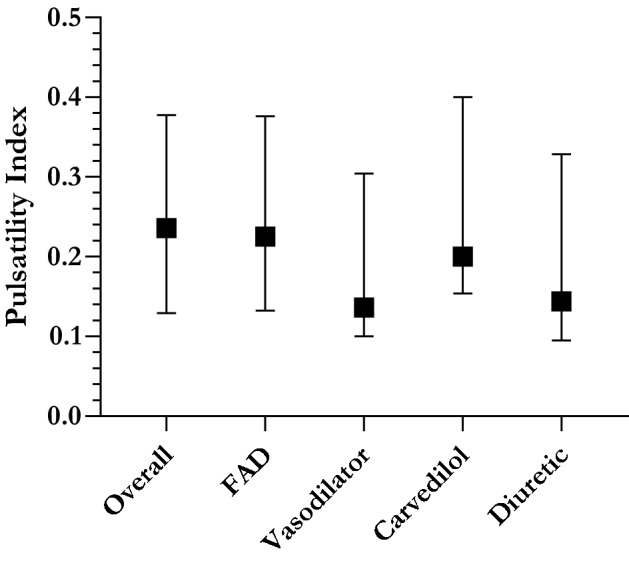
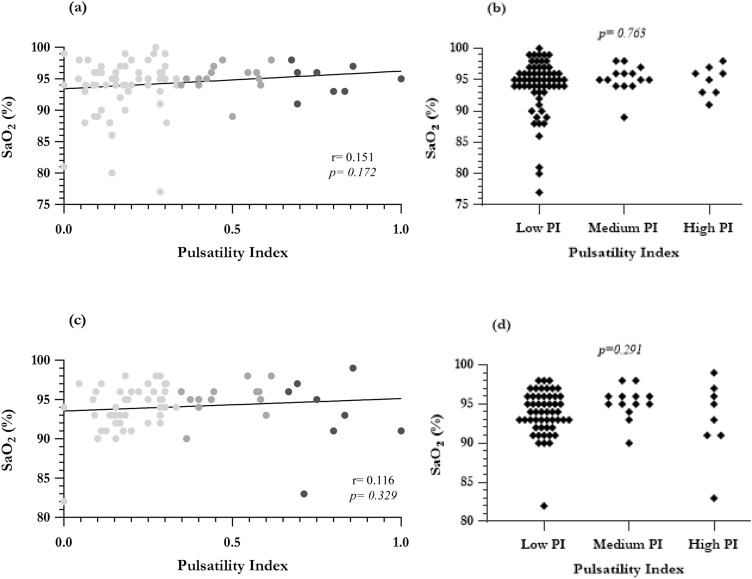
It is unclear whether residual anterograde pulmonary blood flow (APBF) at the time of Fontan is beneficial. Pulsatile pulmonary flow may be important in maintaining a compliant and healthy vascular circuit. We, therefore, wished to ascertain whether there was hemodynamic evidence that residual pulsatile flow at time of Fontan promotes clinical benefit. 106 consecutive children with Fontan completion (1999-2018) were included. Pulmonary artery pulsatility index (PI, (systolic pressure-diastolic pressure)/mean pressure)) was calculated from preoperative cardiac catheterization. Spectral analysis charted PI as a continuum against clinical outcome. The population was subsequently divided into three pulsatility subgroups to facilitate further comparison. Median PI prior to Fontan was 0.236 (range 0-1). 39 had APBF, in whom PI was significantly greater (median: 0.364 vs. 0.177, Mann-Whitney p < 0.0001). There were four early hospital deaths (3.77%), and PI in these patients ranged from 0.214 to 0.423. There was no correlation between PI and standard cardiac surgical outcomes or systemic oxygen saturation at discharge. Median follow-up time was 4.33 years (range 0.0273-19.6), with no late deaths. Increased pulsatility was associated with higher oxygen saturations in the long term, but there was no difference in reported exercise tolerance (Ross), ventricular function, or atrioventricular valve regurgitation at follow-up. PI in those with Fontan-associated complications or the requiring pulmonary vasodilators aligned with the overall population median. Maintenance of pulmonary flow pulsatility did not alter short-term outcomes or long-term prognosis following Fontan although it tended to increase postoperative oxygen saturations, which may be beneficial in later life.
目前尚不清楚在 Fontan 手术时是否存在残余的肺前向血流(APBF)是有益的。脉动性肺血流对于维持顺应性和健康的血管循环可能很重要。因此,我们希望确定在 Fontan 手术时是否存在血流动力学证据表明残余脉动血流可促进临床获益。共纳入 106 例连续接受 Fontan 完成手术的儿童(1999-2018 年)。从术前心导管检查中计算肺动脉搏动指数(PI,(收缩压-舒张压)/平均压)。频谱分析将 PI 作为连续图谱与临床结果进行比较。随后将人群分为三个搏动性亚组,以方便进一步比较。Fontan 术前的中位 PI 为 0.236(范围 0-1)。39 例存在 APBF,其 PI 显著较高(中位数:0.364 与 0.177,Mann-Whitney p<0.0001)。有 4 例患儿在早期住院死亡(3.77%),这些患儿的 PI 范围为 0.214 至 0.423。PI 与标准心脏手术结果或出院时的全身氧饱和度之间无相关性。中位随访时间为 4.33 年(范围 0.0273-19.6),无晚期死亡。长期来看,搏动性增加与更高的氧饱和度相关,但在随访时的运动耐量(Ross)、心室功能或房室瓣反流方面无差异。Fontan 相关并发症或需要肺动脉扩张剂的患者的 PI 与总体人群的中位数一致。维持肺血流搏动性并不能改变 Fontan 术后的短期结果或长期预后,但可能会增加术后氧饱和度,这在以后的生活中可能是有益的。