Department of Radiation Oncology, University of Colorado, Anschutz Medical Campus, Aurora, Colorado, USA.
Département de médecine nucléaire et radiobiologie, Université de Sherbrooke, Sherbrooke, Quebec, Canada.
J Immunother Cancer. 2021 Apr;9(4). doi: 10.1136/jitc-2020-001955.
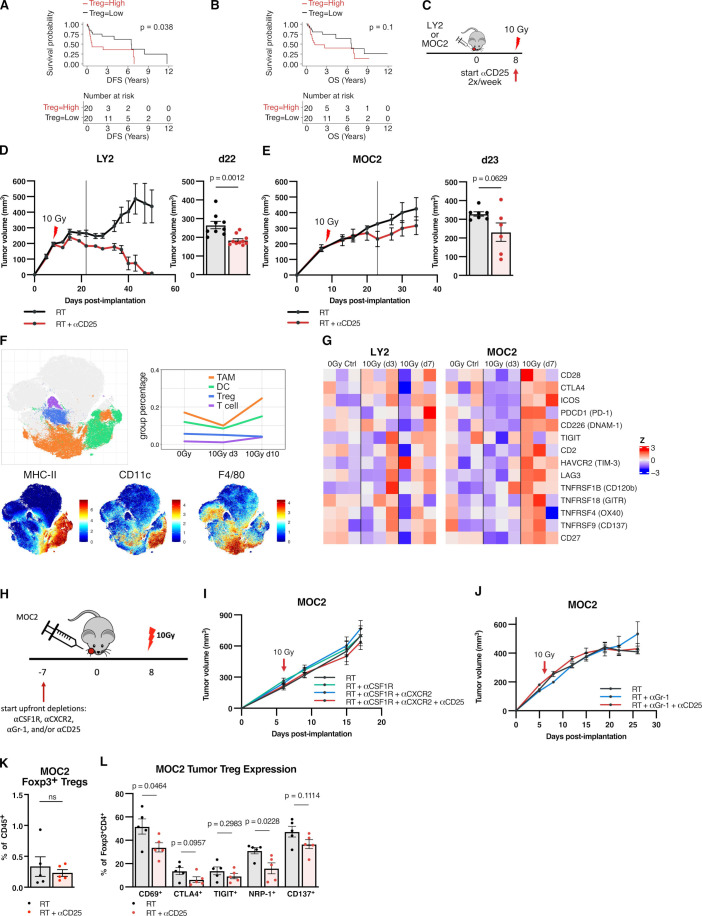
Numerous trials combining radiation therapy (RT) and immunotherapy in head and neck squamous cell carcinoma (HNSCC) are failing. Using preclinical immune cold models of HNSCC resistant to RT-immune checkpoint inhibitors, we investigate therapeutic approaches of overcoming such resistance by examining the differential microenvironmental response to RT.
We subjected two HPV-negative orthotopic mouse models of HNSCC to combination RT, regulatory T cells (Treg) depletion, and/or CD137 agonism. Tumor growth was measured and intratumorous and lymph node immune populations were compared among treatment groups. Human gene sets, genetically engineered mouse models and , flow and time-of-flight cytometry, RNA-Seq, Treg adoptive transfer studies, and in vitro experiments were used to further evaluate the role of dendritic cells (DCs) and Tregs in these treatments.
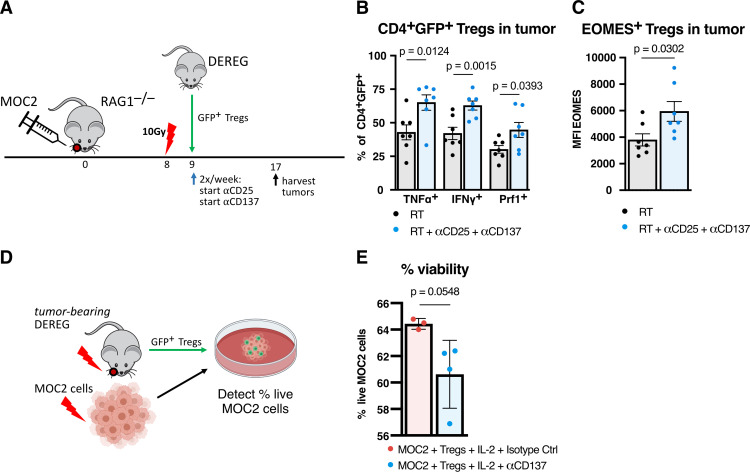
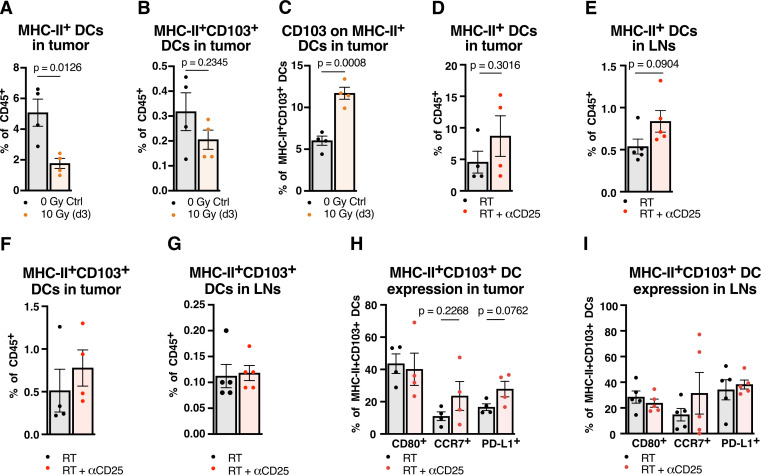
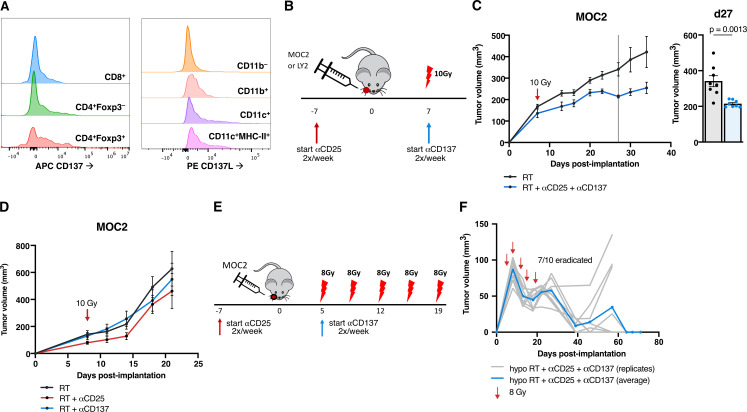
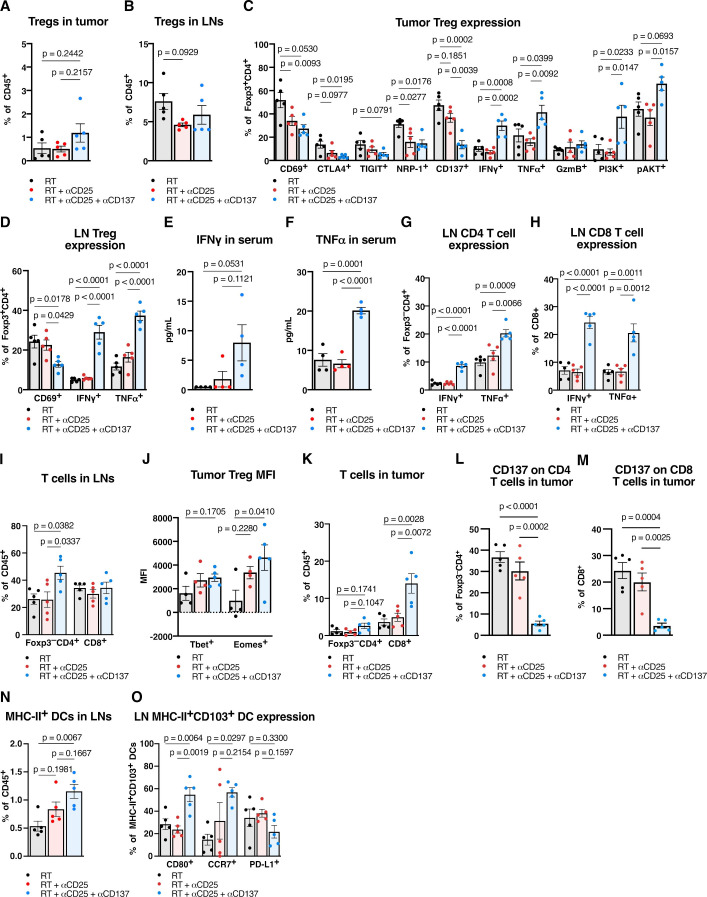
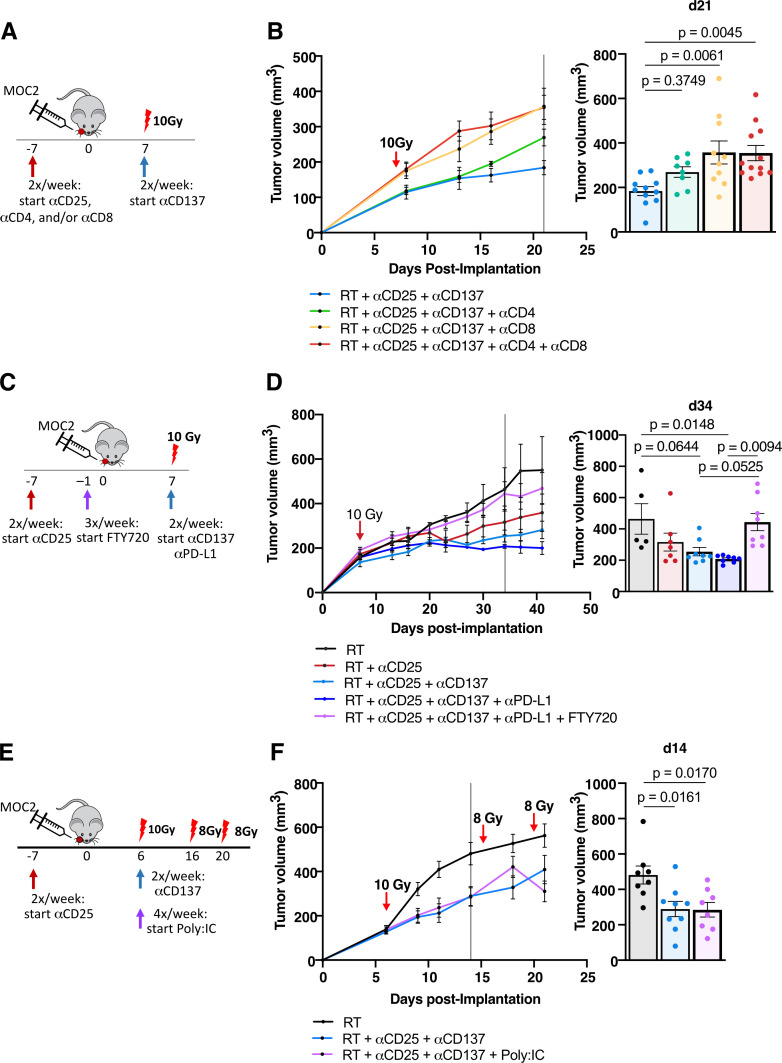
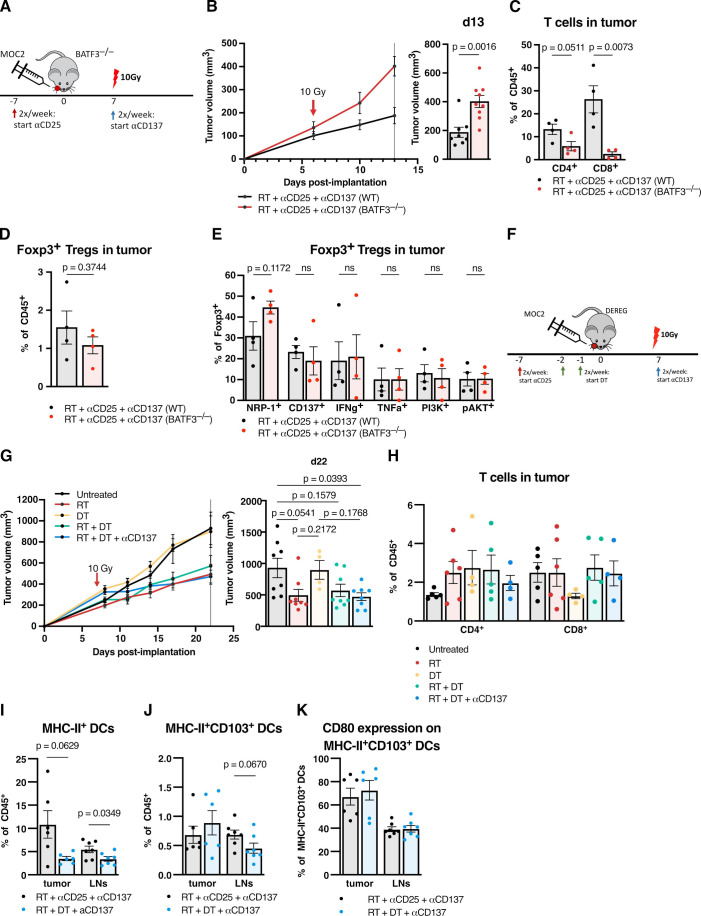
In MOC2 orthotopic tumors, we find no therapeutic benefit to targeting classically defined immunosuppressive myeloids, which increase with RT. In these radioresistant tumors, supplementing combination RT and Treg depletion with anti-CD137 agonism stimulates CD103 DC activation in tumor-draining lymph nodes as characterized by increases in CD80 and CCR7 DCs, resulting in a CD8 T cell-dependent response. Simultaneously, Tregs are reprogrammed to an effector phenotype demonstrated by increases in interferonγ, tumor necrosis factorα, PI3K, pAKT and Eomes populations as well as decreases in CTLA4 and NRP-1 populations. Tumor eradication is observed when RT is increased to an 8 Gy x 5 hypofractionated regimen and combined with anti-CD25+ anti-CD137 treatment. In a human gene set from oral squamous cell carcinoma tumors, high Treg number is associated with earlier recurrence.
Regulating Treg functionality and DC activation status within the lymph node is critical for generating a T cell effector response in these highly radioresistant tumors. These findings underscore the plasticity of Tregs and represent a new therapeutic opportunity for reprogramming the tumor microenvironment in HNSCCs resistant to conventional radioimmunotherapy approaches.
许多将放射治疗(RT)与免疫疗法相结合用于头颈部鳞状细胞癌(HNSCC)的临床试验都失败了。我们使用对 RT-免疫检查点抑制剂有抗性的 HNSCC 临床前免疫冷模型,通过检查对 RT 的不同微环境反应来研究克服这种抗性的治疗方法。
我们使两种 HPV 阴性的 HNSCC 原位小鼠模型接受 RT 联合治疗、调节性 T 细胞(Treg)耗竭和/或 CD137 激动剂治疗。测量肿瘤生长并比较治疗组之间肿瘤内和淋巴结免疫群体。使用人类基因集、基因工程小鼠模型和流式细胞术和飞行时间细胞术、RNA-Seq、Treg 过继转移研究和体外实验进一步评估树突状细胞(DC)和 Tregs 在这些治疗中的作用。
在 MOC2 原位肿瘤中,我们发现针对经典定义的免疫抑制性髓样细胞没有治疗益处,这些细胞随着 RT 而增加。在这些放射抗性肿瘤中,用抗 CD137 激动剂补充 RT 联合 Treg 耗竭可刺激肿瘤引流淋巴结中 CD103 DC 的激活,表现为 CD80 和 CCR7 DC 的增加,导致 CD8 T 细胞依赖性反应。同时,Tregs 被重新编程为效应表型,表现为干扰素γ、肿瘤坏死因子α、PI3K、pAKT 和 Eomes 群体增加,以及 CTLA4 和 NRP-1 群体减少。当 RT 增加到 8 Gy x 5 低分割方案并与抗 CD25+抗 CD137 治疗联合使用时,观察到肿瘤消除。在来自口腔鳞状细胞癌肿瘤的人类基因集中,高 Treg 数量与更早的复发相关。
调节淋巴结中 Treg 的功能和 DC 激活状态对于在这些高度放射抗性肿瘤中产生 T 细胞效应反应至关重要。这些发现强调了 Tregs 的可塑性,并代表了用于重新编程对传统放免治疗方法有抗性的 HNSCC 肿瘤微环境的新治疗机会。