Hospital Universitário Walter Cantídio da Universidade Federal do Ceará (UFC) - Programa de Pós-graduação em Ciências Cardiovasculares da Faculdade de Medicina da UFC, Fortaleza, CE - Brasil.
Universidade Federal do Paraná, Curitiba, PR - Brasil.
Arq Bras Cardiol. 2021 Apr;116(4):814-835. doi: 10.36660/abc.20200420.
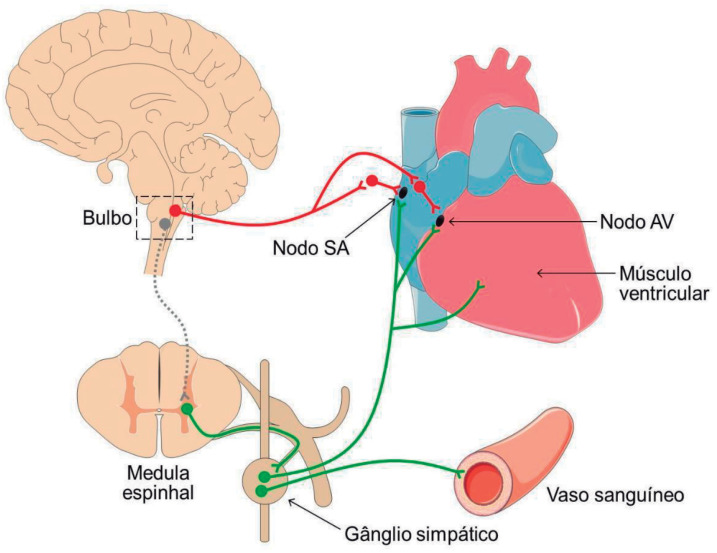
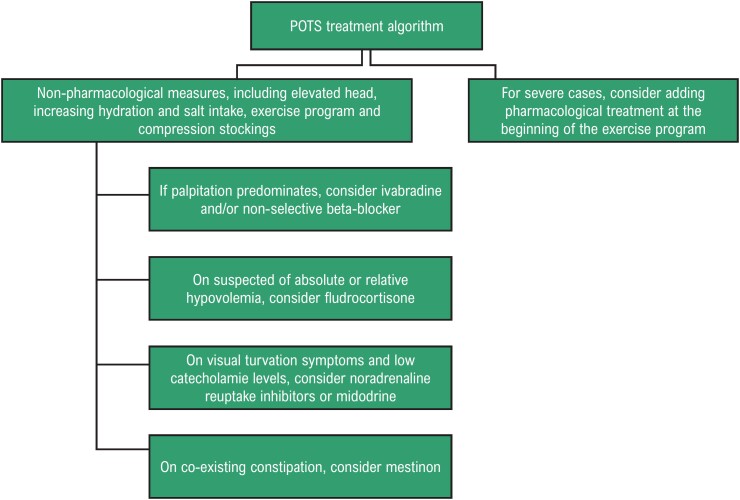
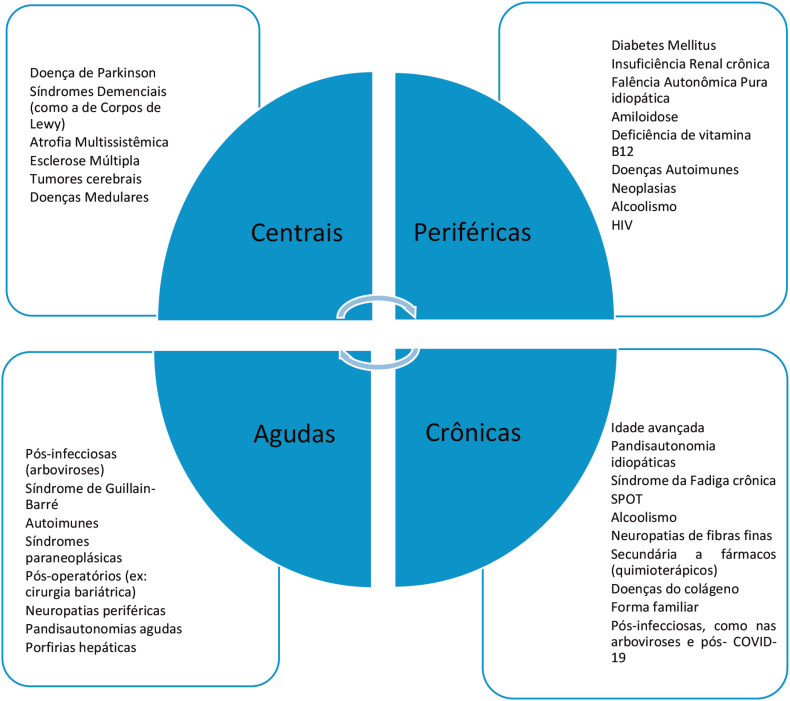
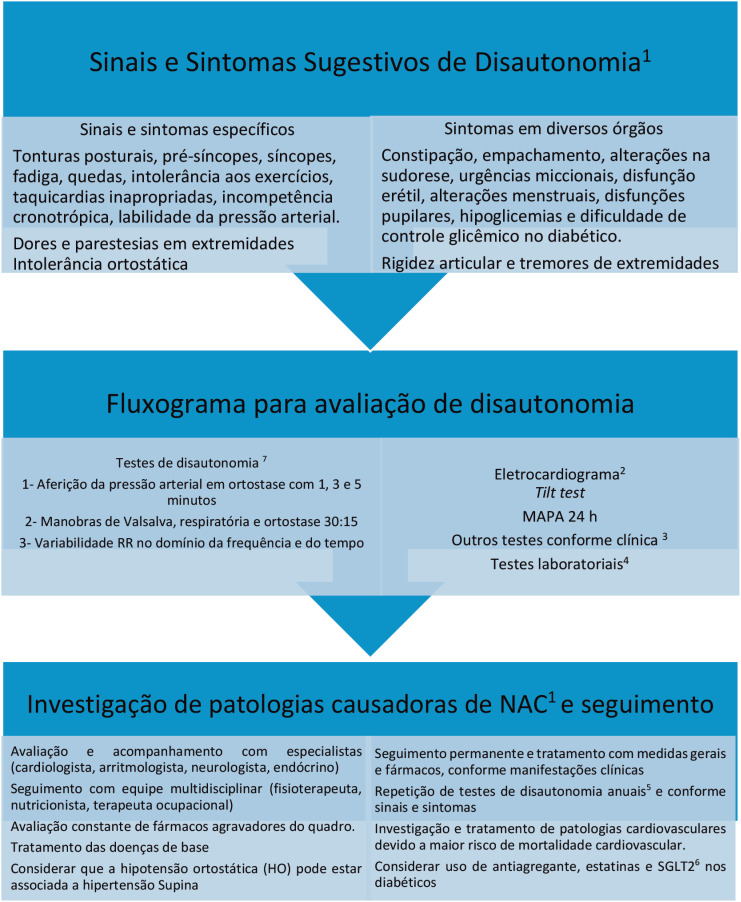
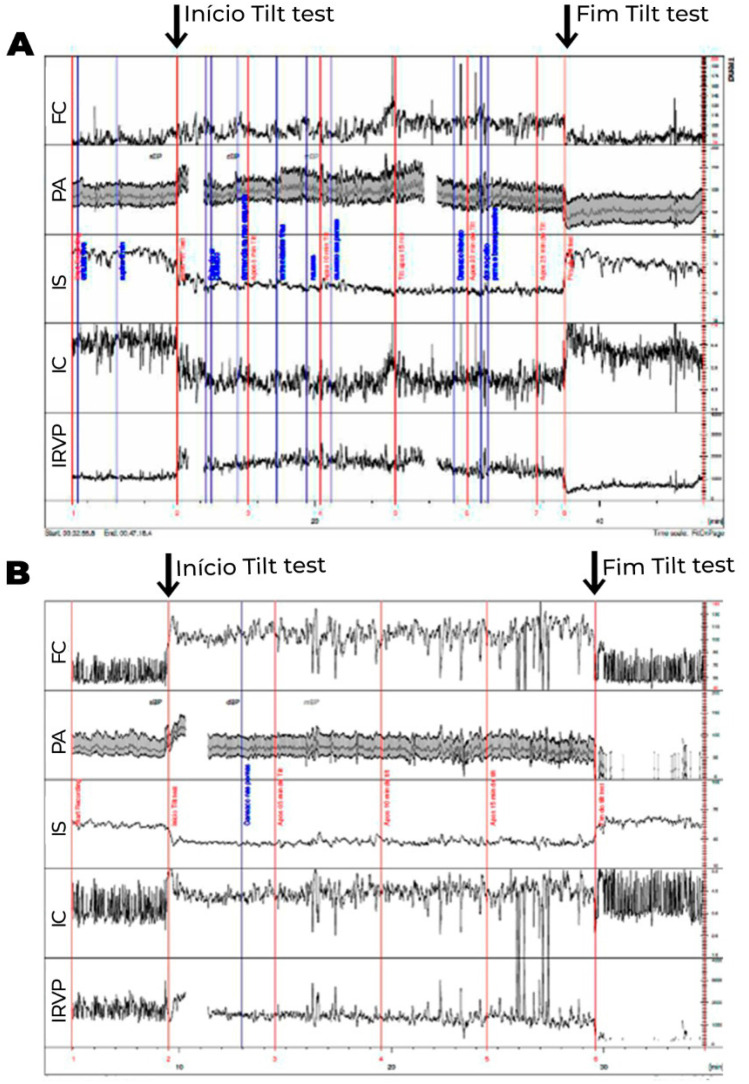
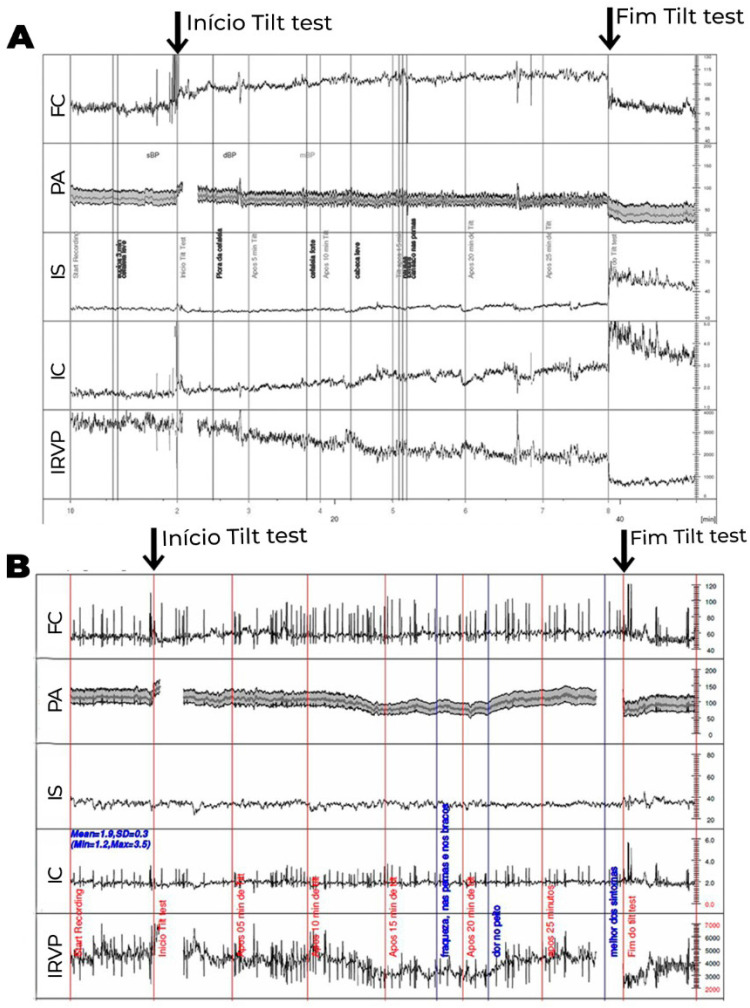
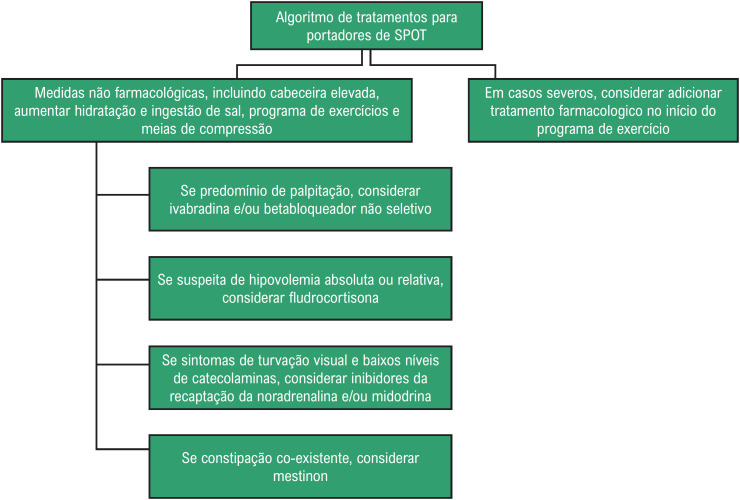
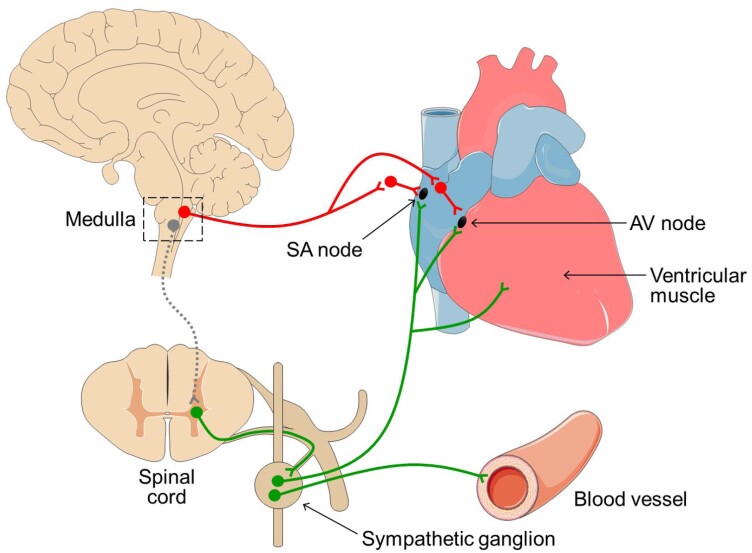
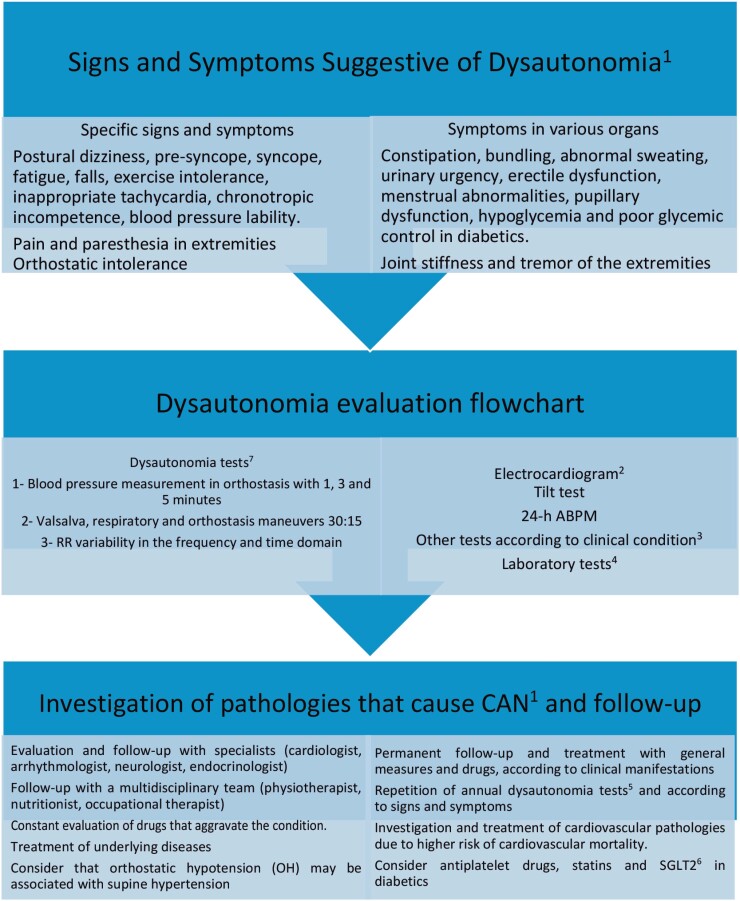
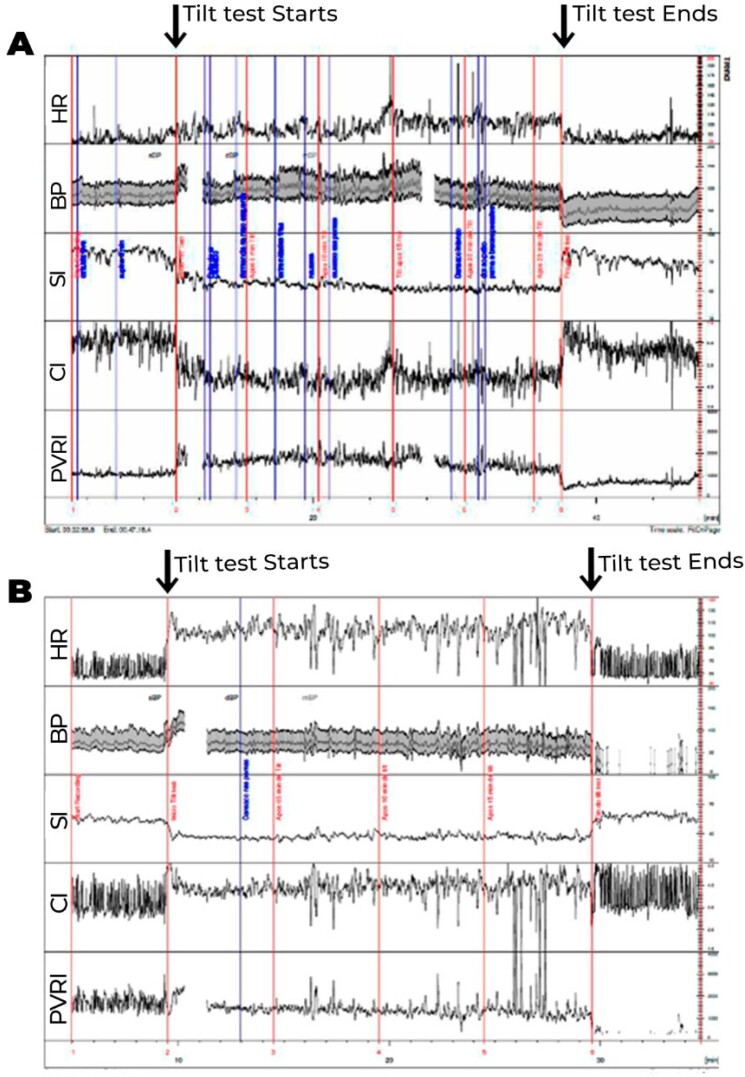
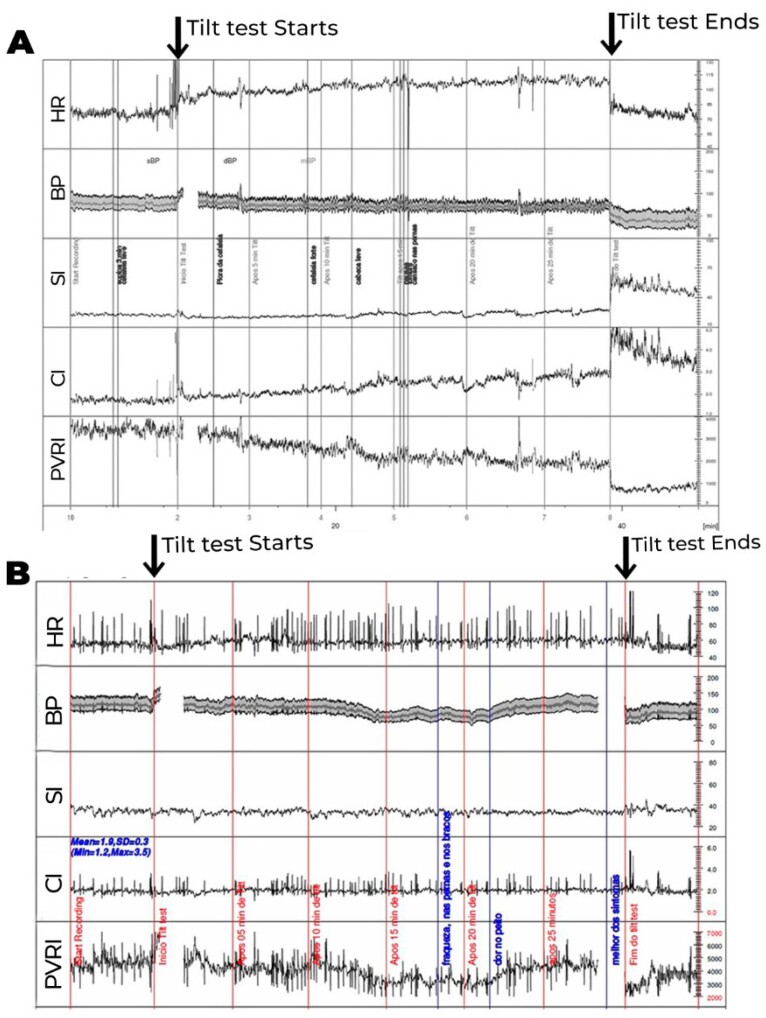
Dysautonomia covers a range of clinical conditions with different characteristics and prognoses. They are classified as Reflex Syndromes, Postural Orthostatic Tachycardia Syndrome (POTS), Chronic Fatigue Syndrome, Neurogenic Orthostatic Hypotension (nOH) and Carotid Sinus Hypersensitivity Syndrome. Reflex (vasovagal) syndromes will not be discussed in this article. Reflex (vasovagal) syndromes are mostly benign and usually occur in patients without an intrinsic autonomic nervous system (ANS) or heart disease. Therefore, they are usually studied separately. Cardiovascular Autonomic Neuropathy (CAN) is the term most currently used to define dysautonomia with impairment of the sympathetic and/or parasympathetic cardiovascular autonomic nervous system. It can be idiopathic, such as multisystemic atrophy or pure autonomic failure, or secondary to systemic pathologies such as diabetes mellitus, neurodegenerative diseases, Parkinson's disease, dementia syndromes, chronic renal failure, amyloidosis and it may also occur in the elderly. The presence of Cardiovascular Autonomic Neuropathy (CAN) implies greater severity and worse prognosis in various clinical situations. Detection of Orthostatic Hypotension (OH) is a late sign and means greater severity in the context of dysautonomia, defined as Neurogenic Orthostatic Hypotension (nOH). It must be differentiated from hypotension due to hypovolemia or medications, called non-neurogenic orthostatic hypotension (nnOH). OH can result from benign causes, such as acute, chronic hypovolemia or use of various drugs. However, these drugs may only reveal subclinical pictures of Dysautonomia. All drugs of patients with dysautonomic conditions should be reevaluated. Precise diagnosis of CAN and the investigation of the involvement of other organs or systems is extremely important in the clinical suspicion of pandysautonomia. In diabetics, in addition to age and time of disease, other factors are associated with a higher incidence of CAN, such poor glycemic control, hypertension, dyslipidemia and obesity. Among diabetic patients, 38-44% can develop Dysautonomia, with prognostic implications and higher cardiovascular mortality. In the initial stages of DM, autonomic dysfunction involves the parasympathetic system, then the sympathetic system and, later on, it presents as orthostatic hypotension. Valsalva, Respiratory and Orthostatic tests (30:15) are the gold standard methods for the diagnosis of CAN. They can be associated with RR Variability tests in the time domain, and mainly in the frequency domain, to increase the sensitivity (protocol of the 7 tests). These tests can detect initial or subclinical abnormalities and assess severity and prognosis. The Tilt Test should not be the test of choice for investigating CAN at an early stage, as it detects cases at more advanced stages. Tilt response with a dysautonomic pattern (gradual drop in blood pressure without increasing heart rate) may suggest CAN. Treatment of patients at moderate to advanced stages of dysautonomia is quite complex and often refractory, requiring specialized and multidisciplinary evaluation. There is no cure for most types of Dysautonomia at a late stage. NOH patients can progress with supine hypertension in more than 50% of the cases, representing a major therapeutic challenge. The immediate risk and consequences of OH should take precedence over the later risks of supine hypertension and values greater than 160/90 mmHg are tolerable. Sleeping with the head elevated (20-30 cm), not getting up at night, taking short-acting antihypertensive drugs for more severe cases, such as losartan, captopril, clonidine or nitrate patches, may be necessary and effective in some cases. Preventive measures such as postural care; good hydration; higher salt intake; use of compression stockings and abdominal straps; portioned meals; supervised physical activity, mainly sitting, lying down or exercising in the water are important treatment steps. Various drugs can be used for symptomatic nOH, especially fludrocortisone, midodrine and droxidopa, the latter not available in Brazil. The risk of exacerbation or triggering supine hypertension should be considered. Chronic Fatigue Syndrome represents a form of Dysautonomia and has been renamed as a systemic disease of exercise intolerance, with new diagnostic criteria: 1 - Unexplained fatigue, leading to occupational disability for more than 6 months; 2 - Feeling ill after exercising; 3 - Non-restorative sleep; 4 - One of the following findings: cognitive impairment or orthostatic intolerance. Several pathologies today have evolved with chronic fatigue, being called chronic diseases associated with chronic fatigue. Postural orthostatic tachycardia syndrome (POTS), another form of presentation of dysautonomic syndromes, is characterized by sustained elevation of heart rate (HR) ≥30 bpm (≥40 bpm if <20 years) or HR ≥120 bpm, in the first 10 minutes in an orthostatic position or during the tilt test, without classical orthostatic hypotension associated. A slight decrease in blood pressure may occur. Symptoms appear or get worse in an orthostatic position, with dizziness, weakness, pre-syncope, palpitations, and other systemic symptoms being common.
自主神经功能障碍涵盖了一系列具有不同特征和预后的临床情况。它们可分为反射性综合征、体位性心动过速综合征(POTS)、慢性疲劳综合征、神经源性直立性低血压(nOH)和颈动脉窦过敏综合征。本文将不讨论反射性(血管迷走性)综合征。反射性(血管迷走性)综合征大多为良性,通常发生在没有内在自主神经系统(ANS)或心脏病的患者中。因此,它们通常单独研究。心血管自主神经病变(CAN)是目前最常用于定义自主神经功能障碍伴交感和/或副交感心血管自主神经功能损害的术语。它可以是特发性的,如多系统萎缩或单纯自主神经衰竭,也可以是继发于糖尿病、神经退行性疾病、帕金森病、痴呆综合征、慢性肾衰竭、淀粉样变性等系统性疾病,也可能发生在老年人中。心血管自主神经病变(CAN)的存在意味着在各种临床情况下严重程度更高,预后更差。直立性低血压(OH)的出现是自主神经功能障碍的晚期征象,意味着神经源性直立性低血压(nOH)的严重程度更高。它必须与由于血容量不足或药物引起的低血压区分开来,称为非神经源性直立性低血压(nnOH)。OH 可能由良性原因引起,如急性、慢性血容量不足或使用各种药物。然而,这些药物可能仅揭示了自主神经功能障碍的亚临床表现。所有患有自主神经功能障碍的患者的药物都应重新评估。在怀疑 pandysautonomia 时,准确诊断 CAN 并调查其他器官或系统的受累情况非常重要。在糖尿病患者中,除了年龄和患病时间外,其他因素与更高的 CAN 发生率相关,如血糖控制不佳、高血压、血脂异常和肥胖。在糖尿病患者中,38-44%可能会发展为自主神经功能障碍,这具有预后意义,并且心血管死亡率更高。在 DM 的早期阶段,自主功能障碍涉及副交感神经系统,然后是交感神经系统,随后表现为直立性低血压。瓦尔萨尔瓦、呼吸和直立位试验(30:15)是 CAN 诊断的金标准方法。它们可以与时间域中的 RR 变异性测试相关联,主要是在频域中,以提高敏感性(7 项测试的方案)。这些测试可以检测到初始或亚临床异常,并评估严重程度和预后。在早期阶段,倾斜试验不应该是调查 CAN 的首选测试,因为它检测到更晚期的病例。直立倾斜试验的自主神经功能障碍模式(血压逐渐下降而心率不增加)可能提示存在 CAN。中重度自主神经功能障碍患者的治疗非常复杂,往往难以治疗,需要进行专门的多学科评估。大多数晚期自主神经功能障碍类型都没有治愈方法。在超过 50%的情况下,nOH 患者可能会进展为仰卧位高血压,这是一个主要的治疗挑战。OH 的即时风险和后果应优先于仰卧位高血压的后期风险,并且 160/90mmHg 以上的血压是可以耐受的。使用头高位(20-30 厘米)睡觉、夜间不起床、在更严重的情况下使用短效降压药,如氯沙坦、卡托普利、可乐定或硝酸酯贴片,在某些情况下可能是必要和有效的。预防措施如姿势护理、良好的水化、增加盐的摄入、使用压缩袜和腹部带、分餐、监督下的体育活动,主要是坐着、躺着或在水中锻炼,都是重要的治疗步骤。各种药物可用于治疗症状性 nOH,特别是氟氢可的松、米多君和羟苯丙氨酸,后者在巴西不可用。应考虑加重或引发仰卧位高血压的风险。慢性疲劳综合征代表了一种自主神经功能障碍的形式,已更名为运动不耐受的系统性疾病,具有新的诊断标准:1 - 不明原因的疲劳,导致职业残疾超过 6 个月;2 - 运动后不适;3 - 非恢复性睡眠;4 - 以下发现之一:认知障碍或直立不耐受。今天有许多疾病与慢性疲劳相关,被称为慢性疾病相关的慢性疲劳。体位性心动过速综合征(POTS)是另一种自主神经功能障碍的表现形式,其特征是在直立位或倾斜试验的最初 10 分钟内,心率持续升高≥30 bpm(如果年龄<20 岁,则≥40 bpm)或心率≥120 bpm,而无典型的直立性低血压相关。血压可能会略有下降。症状出现在直立位或恶化,头晕、虚弱、先兆晕厥、心悸和其他全身症状常见。