Gynecologic Oncology Group Foundation (GOG-F) and Stephenson Cancer Center at the University of Oklahoma Health Sciences Center, Oklahoma City, OK.
Sarah Cannon Research Institute, Nashville, TN.
J Clin Oncol. 2021 Jun 10;39(17):1842-1855. doi: 10.1200/JCO.21.00306. Epub 2021 Apr 23.
To evaluate the addition of the humanized monoclonal antiprogrammed death ligand-1 (PD-L1) antibody, atezolizumab, to platinum-based chemotherapy and bevacizumab in newly diagnosed stage III or IV ovarian cancer (OC).
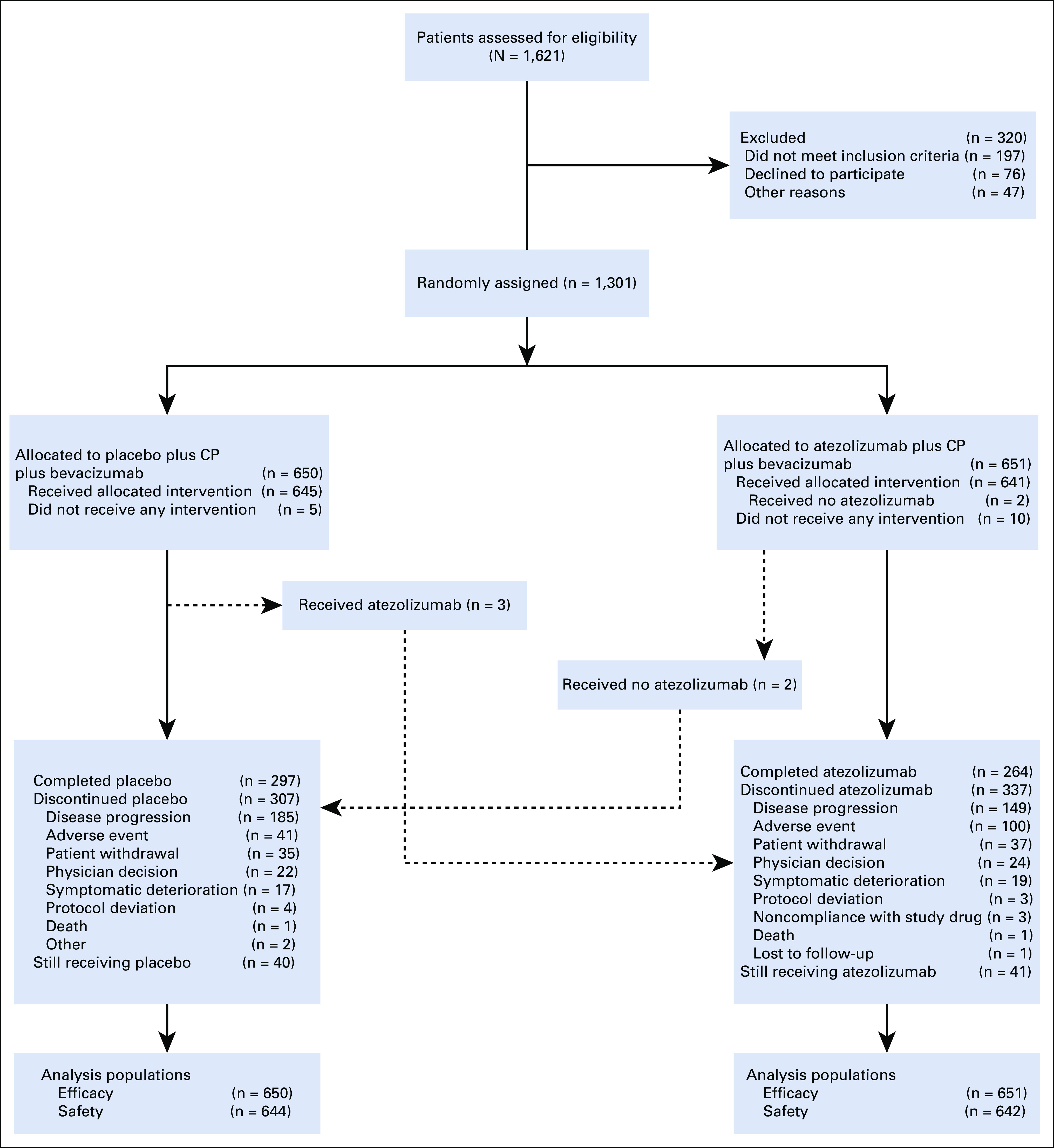
This multicenter placebo-controlled double-blind randomized phase III trial (ClinicalTrials.gov identifier: NCT03038100) enrolled patients with newly diagnosed untreated International Federation of Gynecology and Obstetrics (FIGO) stage III or IV OC who either had undergone primary cytoreductive surgery with macroscopic residual disease or were planned to receive neoadjuvant chemotherapy and interval surgery. Patients were stratified by FIGO stage, Eastern Cooperative Oncology Group performance status, tumor immune cell PD-L1 staining, and treatment strategy and randomly assigned 1:1 to receive 3-weekly cycles of atezolizumab 1,200 mg or placebo (day 1, cycles 1-22), with paclitaxel plus carboplatin (day 1, cycles 1-6) plus bevacizumab 15 mg/kg (day 1, cycles 2-22), omitting perioperative bevacizumab in neoadjuvant patients. The co-primary end points were investigator-assessed progression-free survival and overall survival in the intention-to-treat and PD-L1-positive populations.
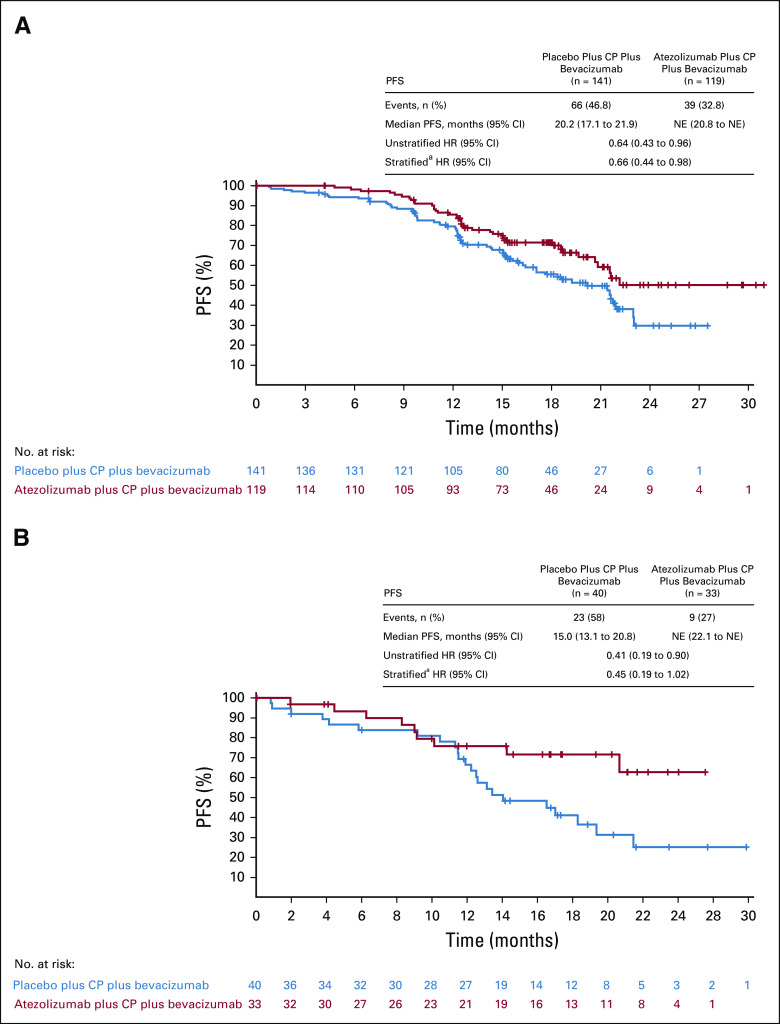
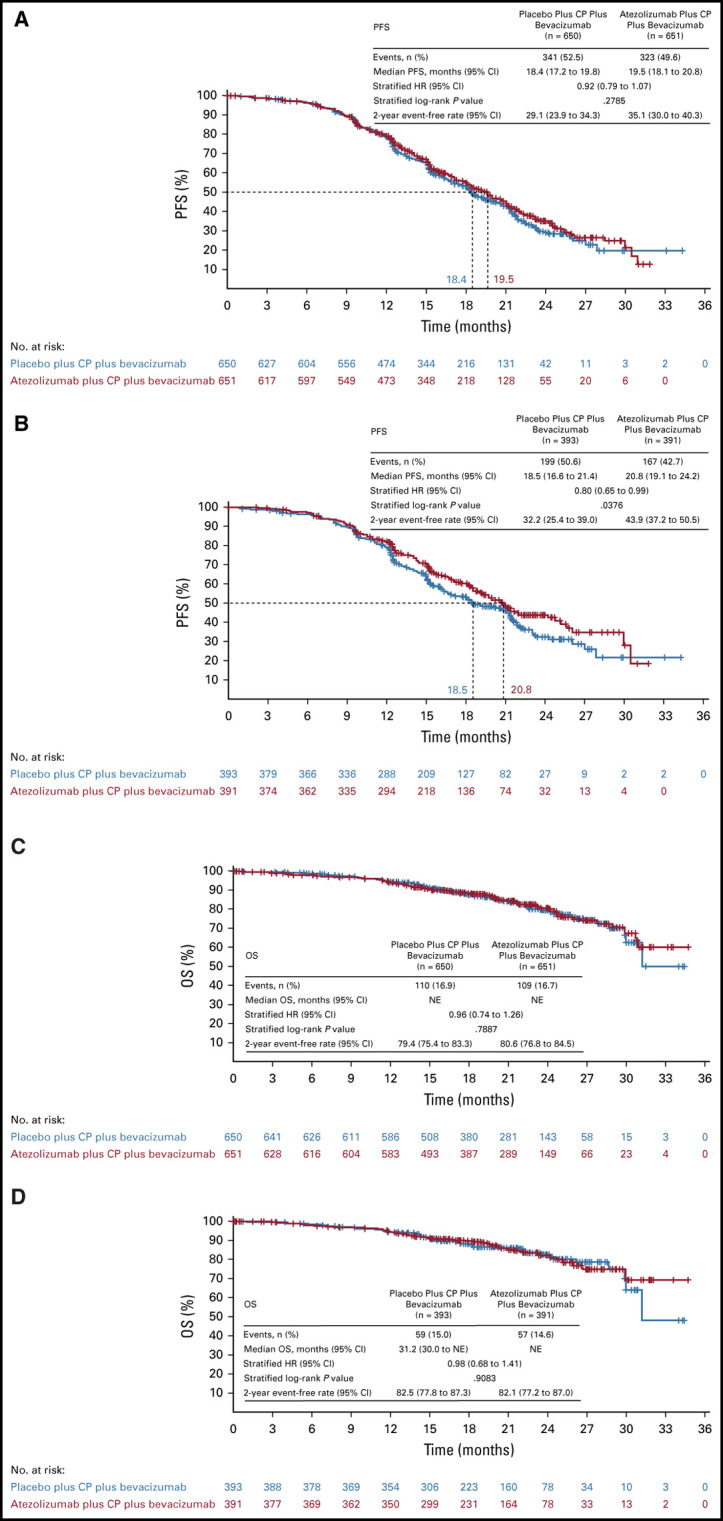
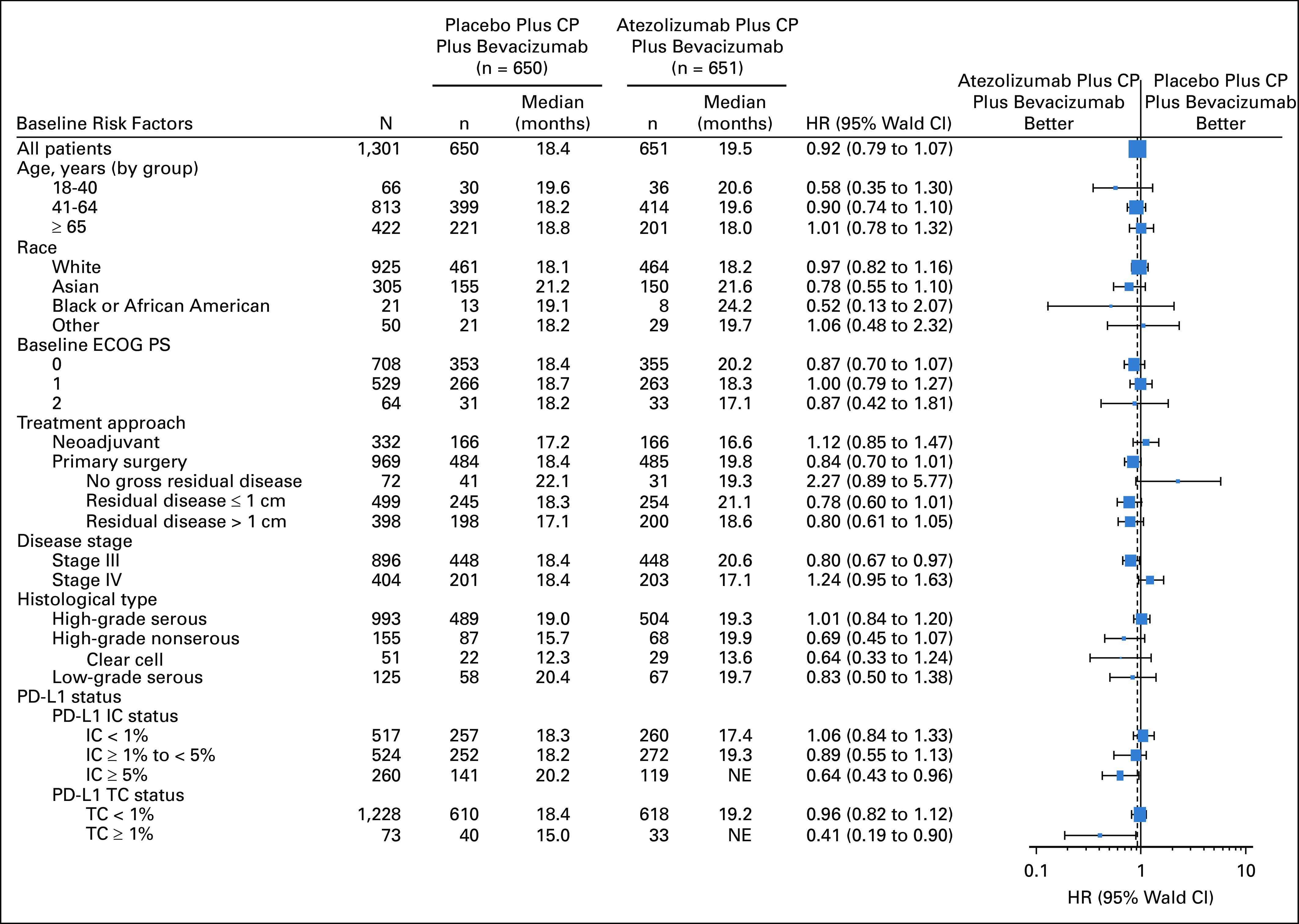
Between March 8, 2017, and March 26, 2019, 1,301 patients were enrolled. The median progression-free survival was 19.5 versus 18.4 months with atezolizumab versus placebo, respectively (hazard ratio, 0.92; 95% CI, 0.79 to 1.07; stratified log-rank = .28), in the intention-to-treat population and 20.8 versus 18.5 months, respectively (hazard ratio, 0.80; 95% CI, 0.65 to 0.99; = .038), in the PD-L1-positive population. The interim (immature) overall survival results showed no significant benefit from atezolizumab. The most common grade 3 or 4 adverse events were neutropenia (21% with atezolizumab 21% with placebo), hypertension (18% 20%, respectively), and anemia (12% 12%).
Current evidence does not support the use of immune checkpoint inhibitors in newly diagnosed OC. Insight from this trial should inform further evaluation of immunotherapy in OC.
评估人源化单克隆抗程序性死亡配体-1(PD-L1)抗体阿替利珠单抗联合铂类化疗和贝伐珠单抗在新诊断的 III 期或 IV 期卵巢癌(OC)中的作用。
这是一项多中心安慰剂对照、双盲、随机 III 期临床试验(ClinicalTrials.gov 标识符:NCT03038100),纳入了新诊断为未经治疗的国际妇产科联合会(FIGO)III 期或 IV 期 OC 的患者,这些患者要么接受了有明确残留病灶的初次细胞减灭术,要么计划接受新辅助化疗和间隔手术。患者按 FIGO 分期、东部合作肿瘤学组表现状态、肿瘤免疫细胞 PD-L1 染色和治疗策略进行分层,并以 1:1 的比例随机分配接受每周 3 次的阿替利珠单抗 1200mg 或安慰剂(第 1 天,第 1-22 周期),联合紫杉醇加卡铂(第 1 天,第 1-6 周期)加贝伐珠单抗 15mg/kg(第 1 天,第 2-22 周期),新辅助治疗患者中省略围手术期贝伐珠单抗。主要研究终点是意向治疗人群和 PD-L1 阳性人群中研究者评估的无进展生存期和总生存期。
2017 年 3 月 8 日至 2019 年 3 月 26 日期间,共纳入 1301 例患者。阿替利珠单抗组和安慰剂组的中位无进展生存期分别为 19.5 个月和 18.4 个月(风险比,0.92;95%CI,0.79 至 1.07;分层对数秩检验 =.28),在意向治疗人群中;分别为 20.8 个月和 18.5 个月(风险比,0.80;95%CI,0.65 至 0.99; =.038),在 PD-L1 阳性人群中。中期(不成熟)总生存期结果显示阿替利珠单抗无显著获益。最常见的 3 级或 4 级不良事件是中性粒细胞减少(阿替利珠单抗组 21%,安慰剂组 21%)、高血压(18% 20%,分别)和贫血(12% 12%)。
目前的证据不支持将免疫检查点抑制剂用于新诊断的 OC。本试验的结果应能为 OC 中免疫治疗的进一步评估提供信息。