Department of Medical Oncology, Dr B.R.A.I.R.C.H., All India Institute of Medical Sciences, New Delhi, India.
Department of Radiodiagnosis, Dr B.R.A.I.R.C.H., All India Institute of Medical Sciences, New Delhi, India.
JCO Glob Oncol. 2021 Apr;7:593-601. doi: 10.1200/GO.20.00629.
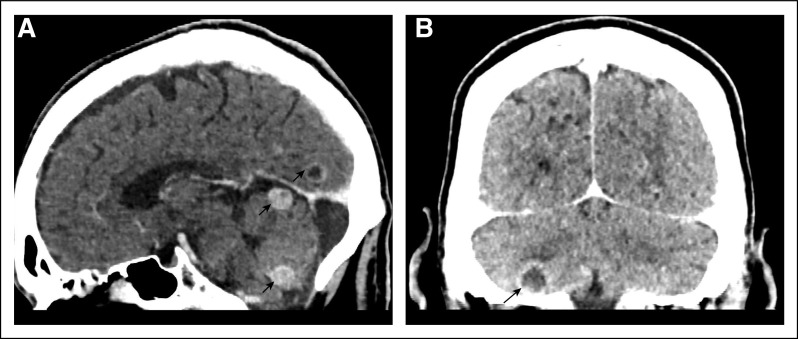
The incidence of symptomatic brain metastasis at diagnosis in non-small-cell lung cancer (NSCLC) is 5%-10%, and up to 40% develop during the disease course. There is a paucity of data supporting the role of brain imaging at diagnosis in asymptomatic cases particularly from resource-constraint settings. Here, we present our experience of mandatory baseline brain imaging with contrast-enhanced computed tomography (CECT) scans of all patients with NSCLC.
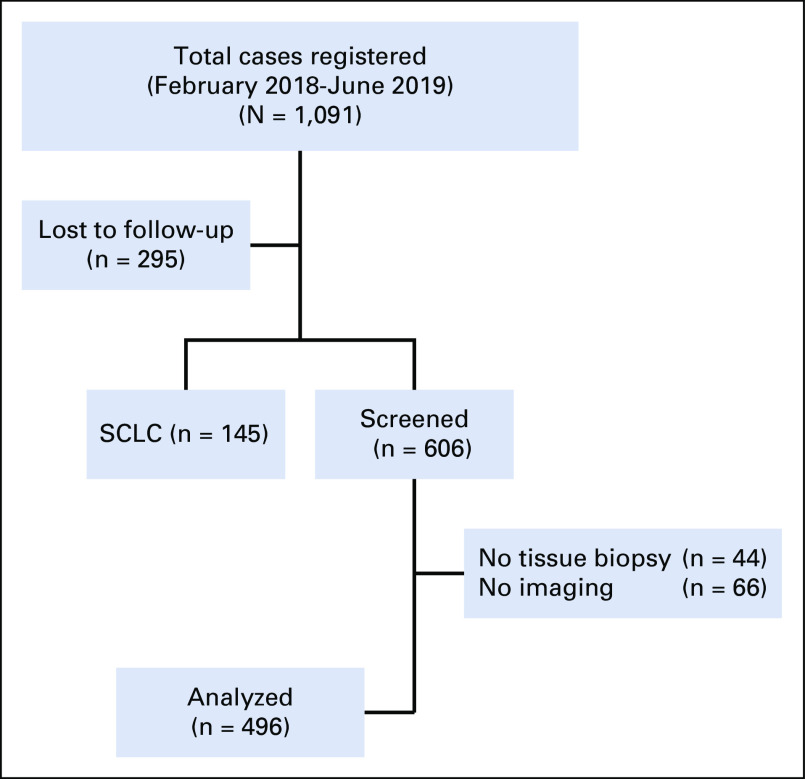
This was a prospective observation study of patients with NSCLC with mandatory baseline brain CECT and a CNS examination. All histology proven patients with NSCLC diagnosed between January 2018 and October 2019 were included irrespective of stage.
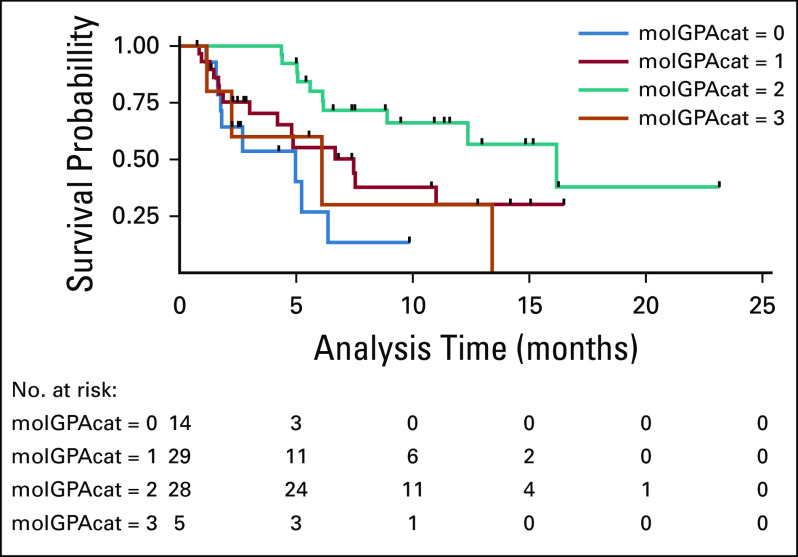
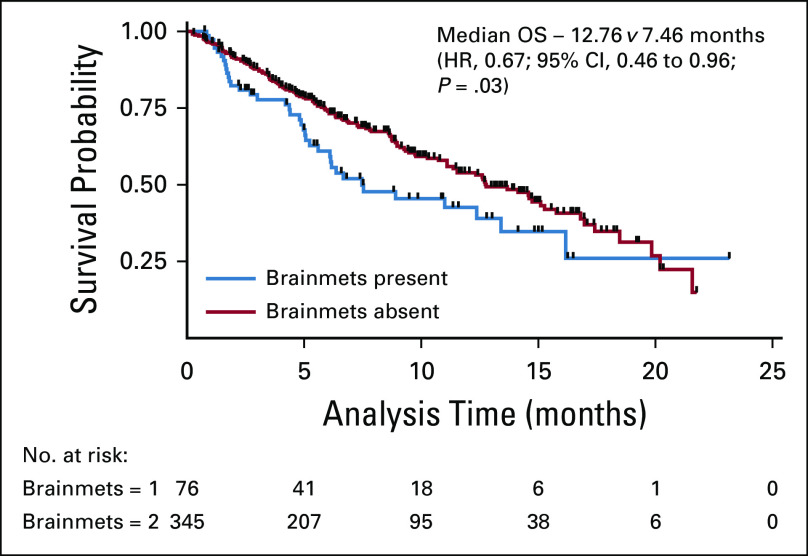
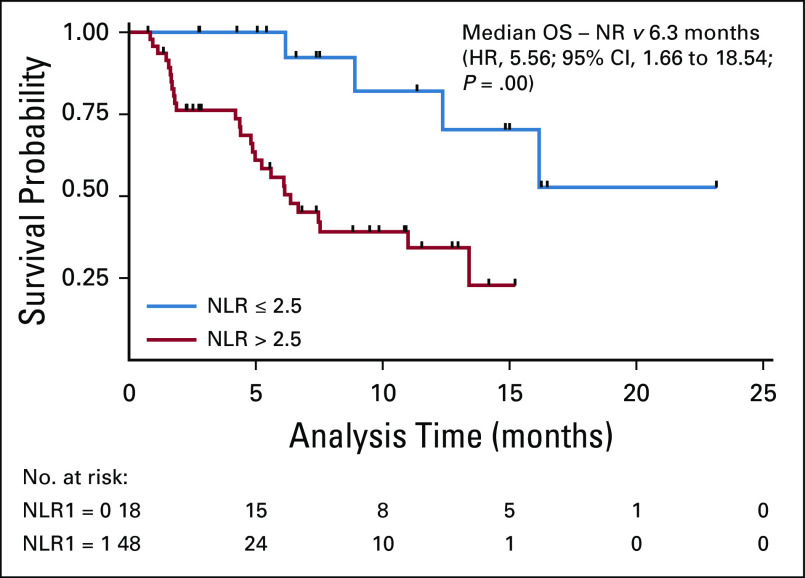
A total of 496 patients were enrolled. The median age was 57 years (range, 23-84) with majority being males (75%) and smokers (66%). The prevalence of epidermal growth factor receptor mutations and anaplastic lymphoma kinase fusions was 33.4% and 12%, respectively. Brain imaging leads to upstaging in 7% cases. The prevalence of brain metastases was 21% (n = 104), with half being asymptomatic (51%). Factors associated with higher proportion of brain metastasis were young age (≤ 40 years), adenocarcinoma histology, poor Eastern Cooperative Oncology Group performance status (3 and 4), and high neutrophil-lymphocyte ratio (NLR) (> 2.5). After a median follow-up of 10.8 months (95% CI, 7.33 to 12.73), the median overall survival was 7.46 versus 12.76 months (hazard ratio 0.67; 95% CI, 0.46 to 0.96; = .03) in patients with and without brain metastases, respectively. On multivariate analyses, high NLR and molecular graded prognostic assessment affected the overall survival significantly.
In our study, 21% of patients had brain metastasis at diagnosis detected with a mandatory baseline brain imaging with CECT. NLR and molecular graded prognostic assessment are significant predictors of survival in patients with brain metastasis.
非小细胞肺癌(NSCLC)患者初诊时出现有症状脑转移的发生率为 5%-10%,多达 40%的患者在疾病过程中出现脑转移。由于资源有限,缺乏支持无症状患者初诊时进行脑影像学检查的相关数据。在此,我们介绍对所有 NSCLC 患者进行强制性基线脑增强 CT(CECT)扫描的经验。
这是一项对所有 NSCLC 患者进行强制性基线脑 CECT 和中枢神经系统检查的前瞻性观察性研究。纳入了 2018 年 1 月至 2019 年 10 月期间确诊的所有组织学证实的 NSCLC 患者,无论分期如何均纳入。
共纳入 496 例患者,中位年龄为 57 岁(范围 23-84 岁),多数为男性(75%)和吸烟者(66%)。表皮生长因子受体突变和间变性淋巴瘤激酶融合的发生率分别为 33.4%和 12%。脑成像导致分期升高的比例为 7%。脑转移的发生率为 21%(n=104),其中一半为无症状(51%)。与脑转移比例较高相关的因素包括年龄较小(≤40 岁)、腺癌组织学、较差的东部肿瘤协作组表现状态(3 和 4 分)和高中性粒细胞-淋巴细胞比值(NLR)(>2.5)。中位随访 10.8 个月(95%CI:7.33-12.73)后,有和无脑转移患者的中位总生存期分别为 7.46 个月和 12.76 个月(风险比 0.67;95%CI:0.46-0.96;P=0.03)。多变量分析显示,高 NLR 和分子分级预后评估对总生存有显著影响。
在我们的研究中,21%的患者通过强制性基线脑 CECT 检查发现初诊时存在脑转移。NLR 和分子分级预后评估是脑转移患者生存的重要预测因素。