Medical School, University of East Anglia, Norwich, UK.
University of Newcastle Upon Tyne, Freeman Hospital, Bone Clinic, Newcastle, UK.
Calcif Tissue Int. 2021 Aug;109(2):157-178. doi: 10.1007/s00223-021-00844-1. Epub 2021 Apr 25.
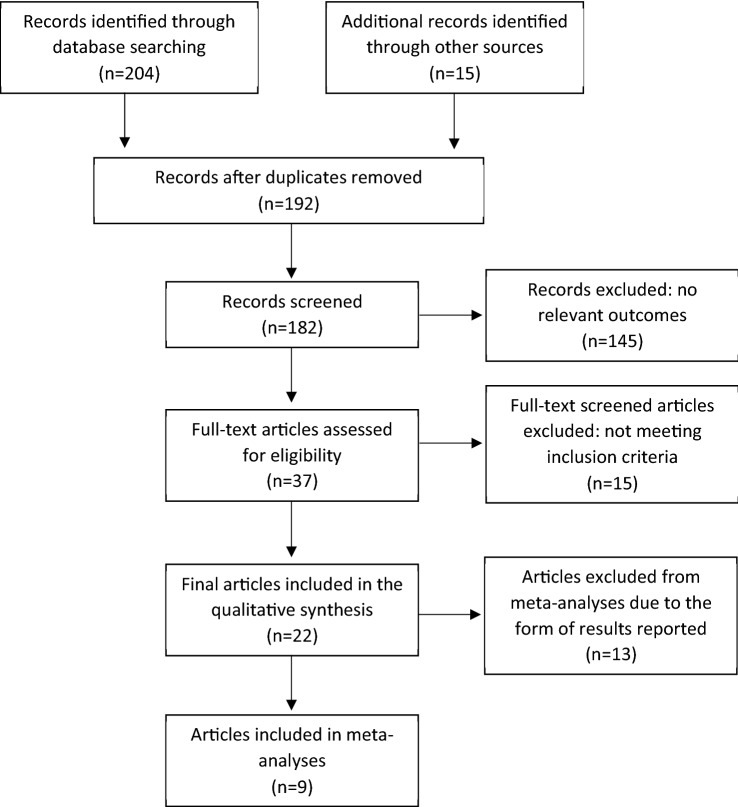
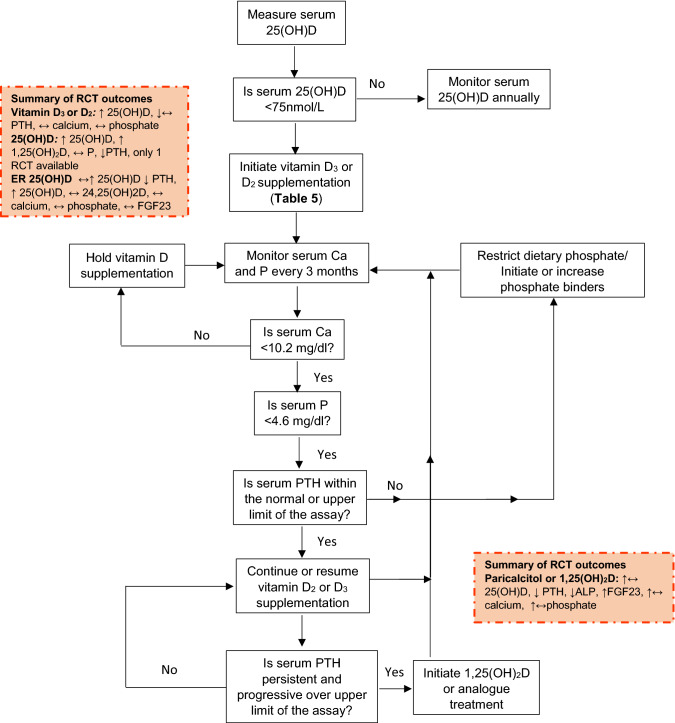
A large proportion of patients with chronic kidney disease (CKD) are vitamin D deficient (plasma 25-hydroxyvitamin D (25(OH)D) < 25 or 30 nmol/L per UK and US population guidelines) and this contributes to the development of CKD-mineral bone disease (CKD-MBD). Gaps in the evidence-base for the management of vitamin D status in relation to CKD-MBD are hindering the formulation of comprehensive guidelines. We conducted a systemic review of 22 RCTs with different forms of vitamin D or analogues with CKD-MBD related outcomes and meta-analyses for parathyroid hormone (PTH). We provide a comprehensive overview of current guidelines for the management of vitamin D status for pre-dialysis CKD patients. Vitamin D supplementation had an inconsistent effect on PTH concentrations and meta-analysis showed non- significant reduction (P = 0.08) whereas calcifediol, calcitriol and paricalcitol consistently reduced PTH. An increase in Fibroblast Growth Factor 23 (FGF23) with analogue administration was found in all 3 studies reporting FGF23, but was unaltered in 4 studies with vitamin D or calcifediol. Few RCTS reported markers of bone metabolism and variations in the range of markers prevented direct comparisons. Guidelines for CKD stages G1-G3a follow general population recommendations. For the correction of deficiency general or CKD-specific patient guidelines provide recommendations. Calcitriol or analogues administration is restricted to stages G3b-G5 and depends on patient characteristics. In conclusion, the effect of vitamin D supplementation in CKD patients was inconsistent between studies. Calcifediol and analogues consistently suppressed PTH, but the increase in FGF23 with calcitriol analogues warrants caution.
很大比例的慢性肾脏病(CKD)患者存在维生素 D 缺乏(根据英国和美国人群指南,血浆 25-羟维生素 D(25(OH)D)<25 或 30nmol/L),这导致了 CKD-矿物质骨病(CKD-MBD)的发生。在 CKD-MBD 相关的维生素 D 状态管理方面,证据基础存在差距,这阻碍了全面指南的制定。我们对 22 项 RCT 进行了系统回顾,这些 RCT 涉及不同形式的维生素 D 或类似物与 CKD-MBD 相关结局,以及甲状旁腺激素(PTH)的 meta 分析。我们提供了一个关于 CKD 患者透析前维生素 D 状态管理的当前指南的全面概述。维生素 D 补充对 PTH 浓度的影响不一致,meta 分析显示无显著降低(P=0.08),而 calcifediol、calcitriol 和 paricalcitol 则一致降低 PTH。所有 3 项报告 FGF23 的研究均发现类似物治疗后 FGF23 增加,但在 4 项维生素 D 或 calcifediol 研究中未改变。很少有 RCT 报告骨代谢标志物,标志物的变化范围阻止了直接比较。G1-G3a 期 CKD 遵循一般人群的建议。对于缺乏的纠正,一般或 CKD 特异性患者指南提供了建议。calcitriol 或类似物的给药仅限于 G3b-G5 期,并且取决于患者的特征。总之,维生素 D 补充在 CKD 患者中的效果在研究之间不一致。Calcifediol 和类似物一致地抑制 PTH,但 calcitriol 类似物增加 FGF23 需要谨慎。