Kim Sunghye, Hsu Fang-Chi, Groban Leanne, Williamson Jeff, Messier Stephen
Department of Internal Medicine, Section of Rheumatology, Wake Forest School of Medicine, Winston-Salem, NC, USA.
Department of Medicine, Section of Rheumatology, W.G. Hefner VA Medical Center, Salisbury, NC, USA.
BMC Musculoskelet Disord. 2021 Apr 26;22(1):388. doi: 10.1186/s12891-021-04253-1.
Knee osteoarthritis (KOA) is increasingly more prevalent and significant number of patients require knee arthroplasty. Although knee arthroplasty is generally successful, it takes months to recover physical function. Preoperative physical function is known to predict postoperative outcomes and exercise can improve preoperative physical function. However, patients with KOA have difficulty exercise on land due to pain and stiffness, while water exercise can be better tolerated. We hypothesized that preoperative water exercise to improve preoperative physical function will improve postoperative outcomes after total knee arthroplasty (TKA).
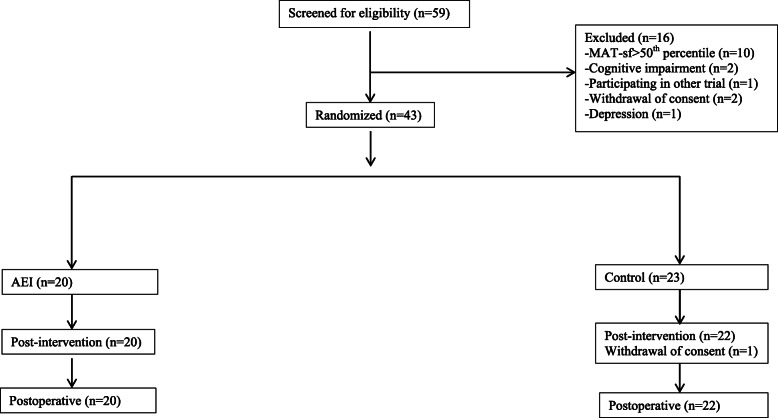
We enrolled 43 participants who were scheduled for elective TKA in 4-8 weeks and scored at or below 50th percentile in mobility assessment tool-sf (MAT-sf). All enrolled participants were assessed on 1) clinical osteoarthritis symptom severity using Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 2) physical function using Short Physical Performance Battery (SPPB), 3) self-reported mobility using Mobility Assessment Tool-short form (MAT-sf), 4) depression using Geriatric Depression Scale-short form (GDS-sf), 5) cognitive function using Montreal Cognitive Assessment (MoCA). Blood samples for high-sensitivity-C-reactive protein (hs-CRP), tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) were stored at - 80 °C then all samples were analyzed together. All the enrolled participants were randomly assigned to the aquatic exercise intervention (AEI) or usual care group. Sixty minute sessions of AEI was conducted three times a week for 4-8 weeks. Participants in both groups were evaluated within 1 week before their scheduled surgery, as well as 4 weeks after the surgery.
The mean age was 67.1 (±6.2), 44% were female, 74% were White. There is no statistically significant difference in combined outcome of any complication, unscheduled ER visit, and disposition to nursing home or rehab facility by AEI. However, AEI was associated with more favorable outcomes: WOMAC scores (p < 0.01), chair-stand (p = 0.019), MAT-sf as well as improved depression (p = 0.043) and cognition (p = 0.008).
4-8 weeks of aquatic exercise intervention resulted in improved functional outcomes as well as improved depression and cognition in elderly patients undergoing TKA. A larger study is warranted to explore the role of water exercise in clinical and functional outcomes of TKA.
膝关节骨关节炎(KOA)越来越普遍,大量患者需要进行膝关节置换术。尽管膝关节置换术总体上是成功的,但恢复身体功能需要数月时间。已知术前身体功能可预测术后结果,运动可以改善术前身体功能。然而,KOA患者由于疼痛和僵硬,在陆地上运动困难,而水上运动耐受性更好。我们假设术前进行水上运动以改善术前身体功能将改善全膝关节置换术(TKA)后的术后结果。
我们招募了43名计划在4至8周内进行择期TKA且在移动性评估工具简表(MAT-sf)中得分处于或低于第50百分位数的参与者。所有入选参与者接受以下评估:1)使用西安大略和麦克马斯特大学骨关节炎指数(WOMAC)评估临床骨关节炎症状严重程度;2)使用简短身体功能量表(SPPB)评估身体功能;3)使用移动性评估工具简表(MAT-sf)进行自我报告的移动性评估;4)使用老年抑郁量表简表(GDS-sf)评估抑郁;5)使用蒙特利尔认知评估量表(MoCA)评估认知功能。采集用于检测高敏C反应蛋白(hs-CRP)、肿瘤坏死因子-α(TNF-α)和白细胞介素-6(IL-6)的血样并储存在-80°C,然后一起分析所有样本。所有入选参与者被随机分配到水上运动干预(AEI)组或常规护理组。AEI每周进行3次,每次60分钟,共进行4至8周。两组参与者在预定手术前1周内以及手术后4周进行评估。
平均年龄为67.1(±6.2)岁,44%为女性,74%为白人。AEI组在任何并发症、非计划急诊就诊以及入住养老院或康复机构的综合结果方面无统计学显著差异。然而,AEI与更有利的结果相关:WOMAC评分(p < 0.01)、从椅子上站起(p = 0.019)、MAT-sf评分,以及抑郁改善(p = 0.043)和认知改善(p = 0.008)。
4至8周的水上运动干预可改善接受TKA的老年患者的功能结果以及抑郁和认知状况。有必要进行更大规模的研究来探讨水上运动在TKA临床和功能结果中的作用。