Department of Urology, Lausanne University Hospital and University of Lausanne, Lausanne, Swizterland.
Departmentof Otolaryngology-Head and Neck Surgery, Lausanne University Hospital and University of Lausanne, Lausanne, Swizterland.
Oncoimmunology. 2021 Apr 13;10(1):1912473. doi: 10.1080/2162402X.2021.1912473.
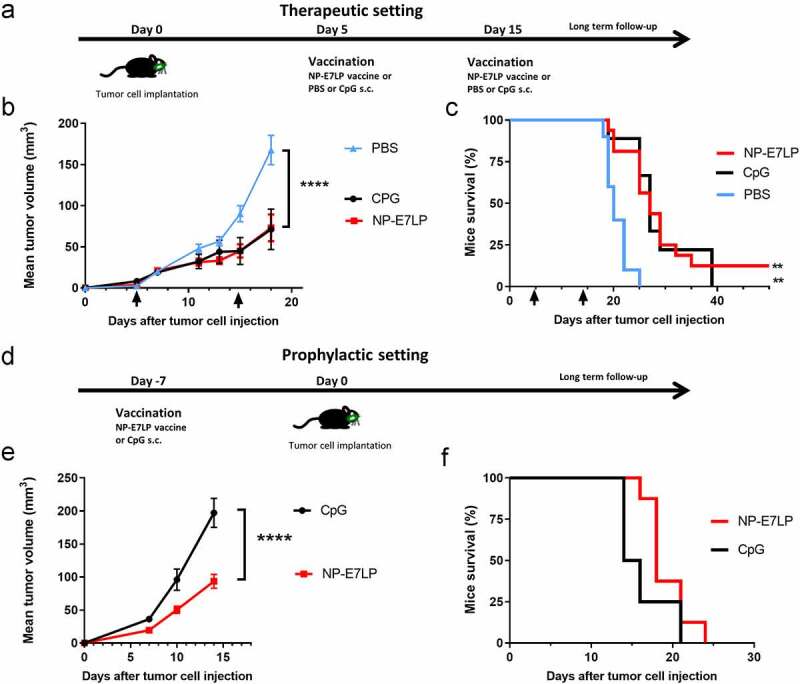
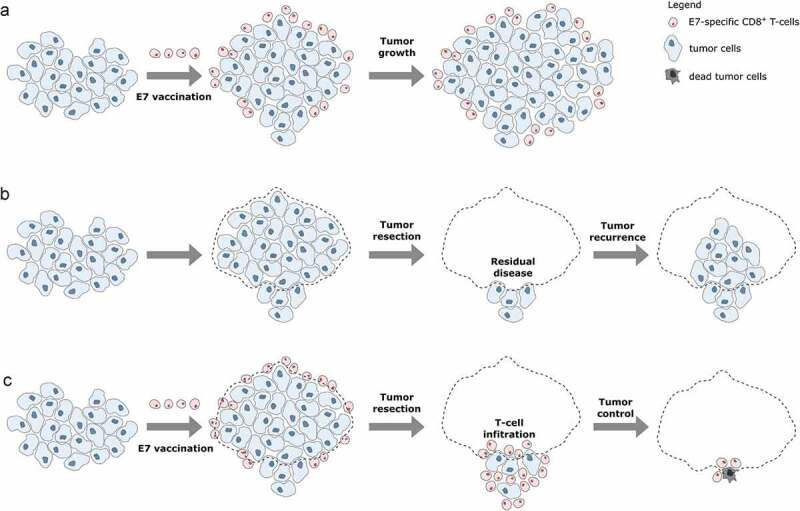
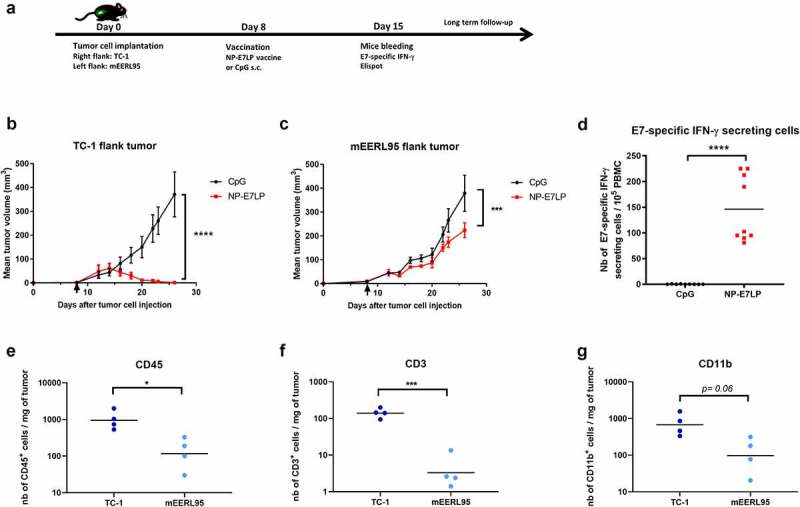
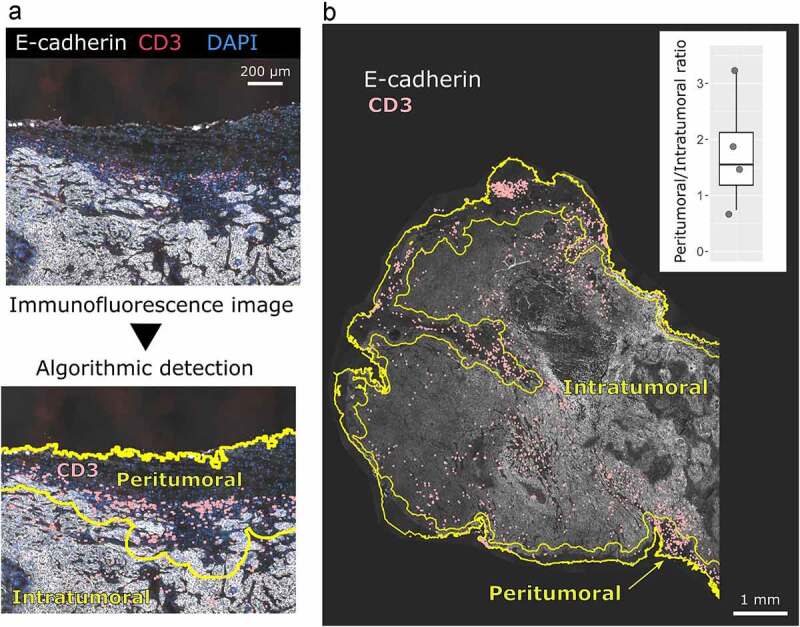
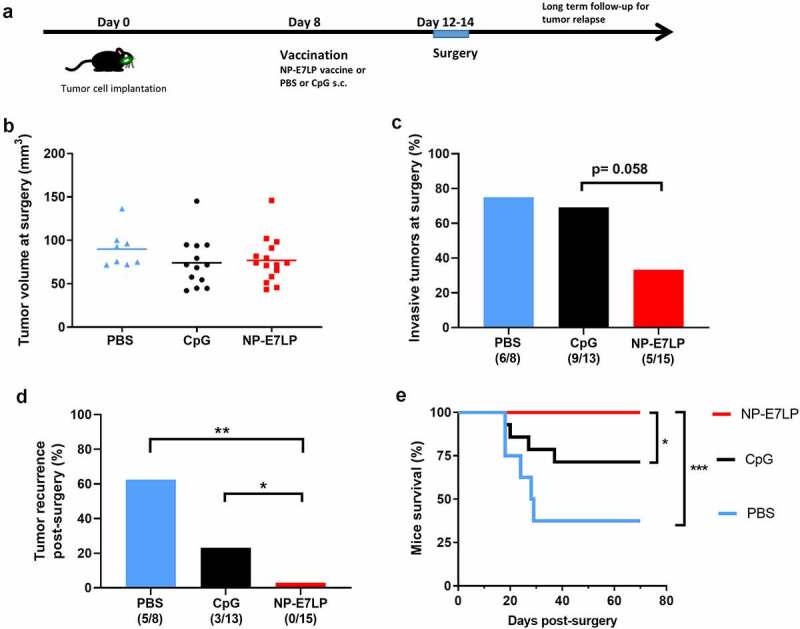
High-risk human papillomavirus (HPV) encoding E6/E7-HPV oncogenes are responsible for a subgroup of head and neck squamous-cell carcinoma (HNSCC) and thus therapeutic E7-vaccines may be used to control HPVHNSCC tumors. Herein we investigated the effects of an optimized nanoparticle-conjugated E7 long-peptide vaccine adjuvanted with CpG (NP-E7LP) in an orthotopic immunocompetent mouse model of HPVHNSCC which is based on injection of HPV16 E6/E7-expressing mEERL95-cells into the submental space. In absence of surgery, vaccination performed before or after tumor-cell injection decreased tumor growth or prolonged mice survival only marginally, despite the high numbers of vaccine-induced circulating E7-specific IFN-γ-secreting CD8 T-cells. This contrasts with the high-efficacy of NP-E7LP-vaccination reported in the genital and subcutaneous HPV16-E6/E7-expressing TC-1 models. Our data show that in a direct comparison, NP-E7LP-vaccination fully controlled TC-1, but not mEERL95, tumors subcutaneously growing in the flanks. Immune-cell infiltration was 10-fold higher in TC-1-tumors, than in mEERL95-tumors, suggesting that vaccine-induced CD8 T-cells can only poorly infiltrate mEERL95-tumors. Indeed, immunofluorescence staining of orthotopic mEERL95-tumors showed that CD3 T-cells are preferentially located peritumorally. However, when NP-E7LP-vaccination was performed after mEERL95-cell injection, but before resection of primary tumors, no postsurgical recurrence was observed and 100% of the mice survived until the experimental endpoint (day 70) in the NP-E7LP-vaccinated group. In contrast, we observed a 60% recurrence rate and only 35% survival in PBS-vaccinated mice. This suggests that removal of the primary tumor modified the tumor microenvironment, allowing a therapeutic effect of the vaccine-induced anti-tumor response. E7-vaccination combined with surgery may thus benefit patients with HPVHNSCC.
高危型人乳头瘤病毒(HPV)编码的 E6/E7-HPV 癌基因是头颈部鳞状细胞癌(HNSCC)亚群的致病因素,因此 E7 疫苗治疗可用于控制 HPV-HNSCC 肿瘤。在此,我们研究了优化的纳米颗粒偶联 E7 长肽疫苗与 CpG(NP-E7LP)联合佐剂在基于 HPV16E6/E7 表达 mEERL95 细胞注射到颏下间隙的 HPV-HNSCC 同源免疫小鼠模型中的作用。在不进行手术的情况下,在肿瘤细胞注射前或后进行疫苗接种仅能轻微减少肿瘤生长或延长小鼠生存时间,尽管疫苗诱导的循环 E7 特异性 IFN-γ 分泌 CD8 T 细胞数量较高。这与 NP-E7LP 疫苗在 HPV16E6/E7 表达的 TC-1 型生殖器和皮下模型中报道的高疗效形成对比。我们的数据表明,在直接比较中,NP-E7LP 疫苗完全控制了 TC-1 但不能控制皮下生长的 mEERL95 肿瘤。TC-1 肿瘤中的免疫细胞浸润比 mEERL95 肿瘤高 10 倍,这表明疫苗诱导的 CD8 T 细胞只能很差地浸润 mEERL95 肿瘤。事实上,对原位 mEERL95 肿瘤的免疫荧光染色显示 CD3 T 细胞优先位于肿瘤周围。然而,当在 mEERL95 细胞注射后但在切除原发性肿瘤之前进行 NP-E7LP 疫苗接种时,在 NP-E7LP 疫苗接种组中未观察到手术后复发,并且 100%的小鼠存活到实验终点(第 70 天)。相比之下,我们在 PBS 疫苗接种组中观察到 60%的复发率和 35%的存活率。这表明原发性肿瘤的切除改变了肿瘤微环境,从而允许疫苗诱导的抗肿瘤反应发挥治疗作用。因此,E7 疫苗接种联合手术可能有益于 HPV-HNSCC 患者。