Department of Surgery, The Transplantation Institute, 2462University of Chicago, Chicago, IL, USA.
Department of Radiology, 2462University of Chicago, Chicago, IL, USA.
Cell Transplant. 2021 Jan-Dec;30:9636897211001774. doi: 10.1177/09636897211001774.
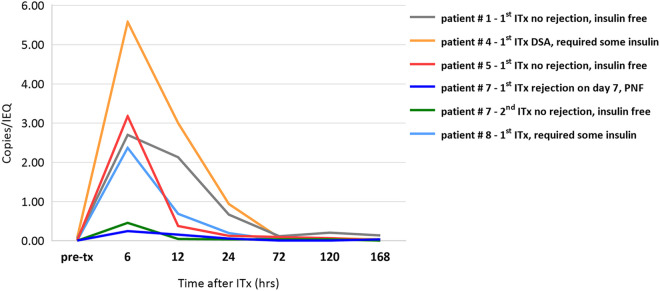
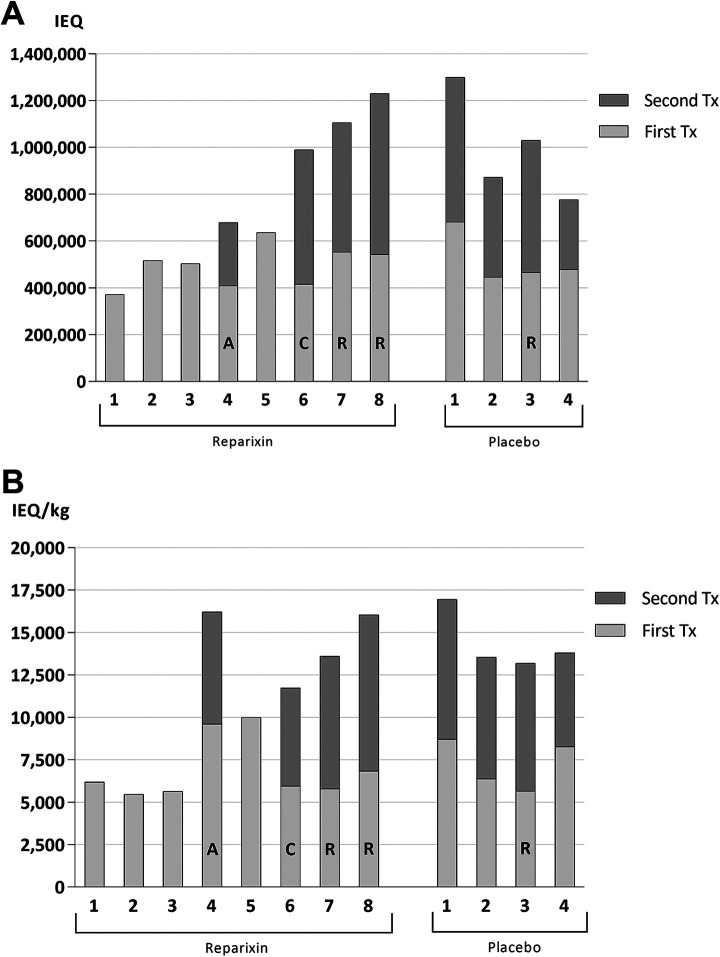
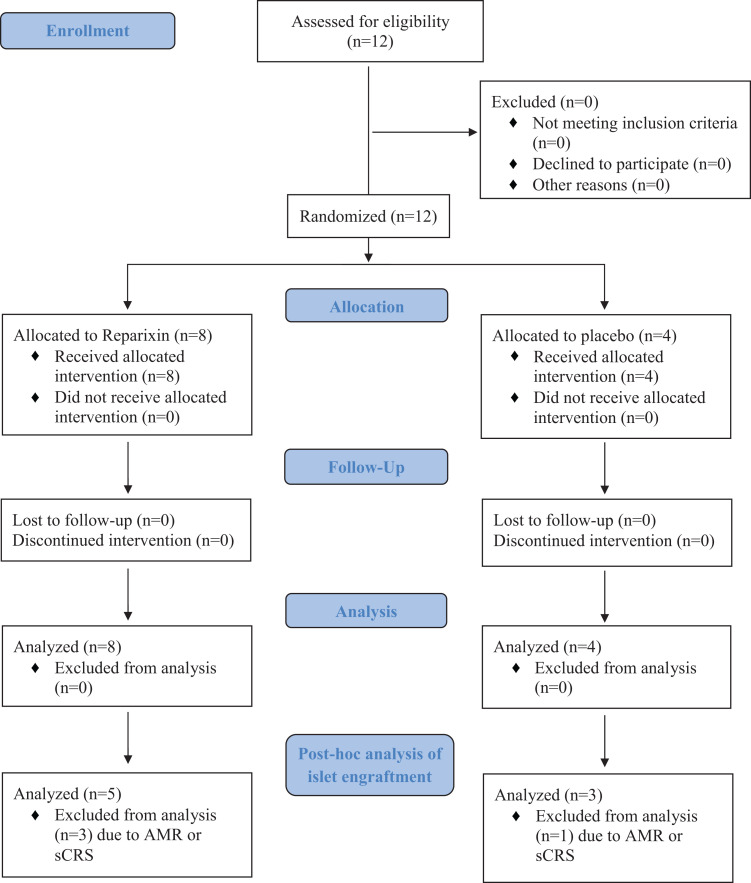
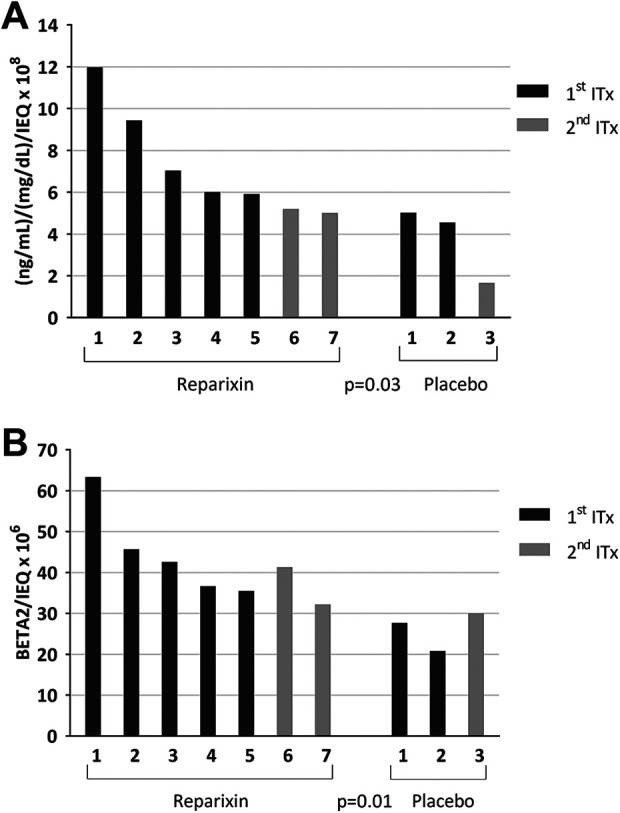
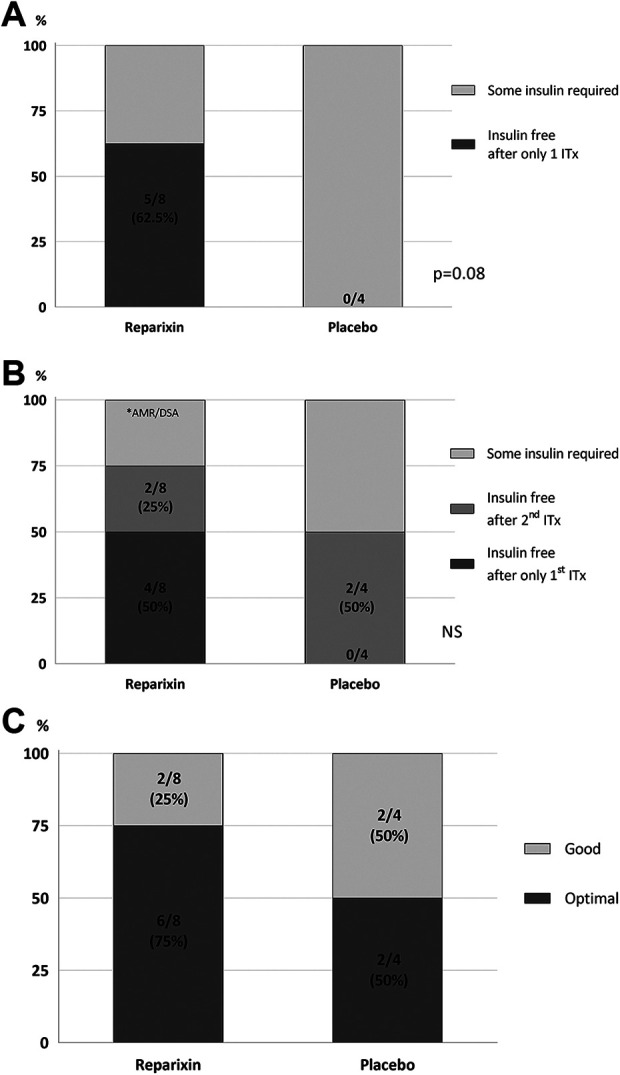
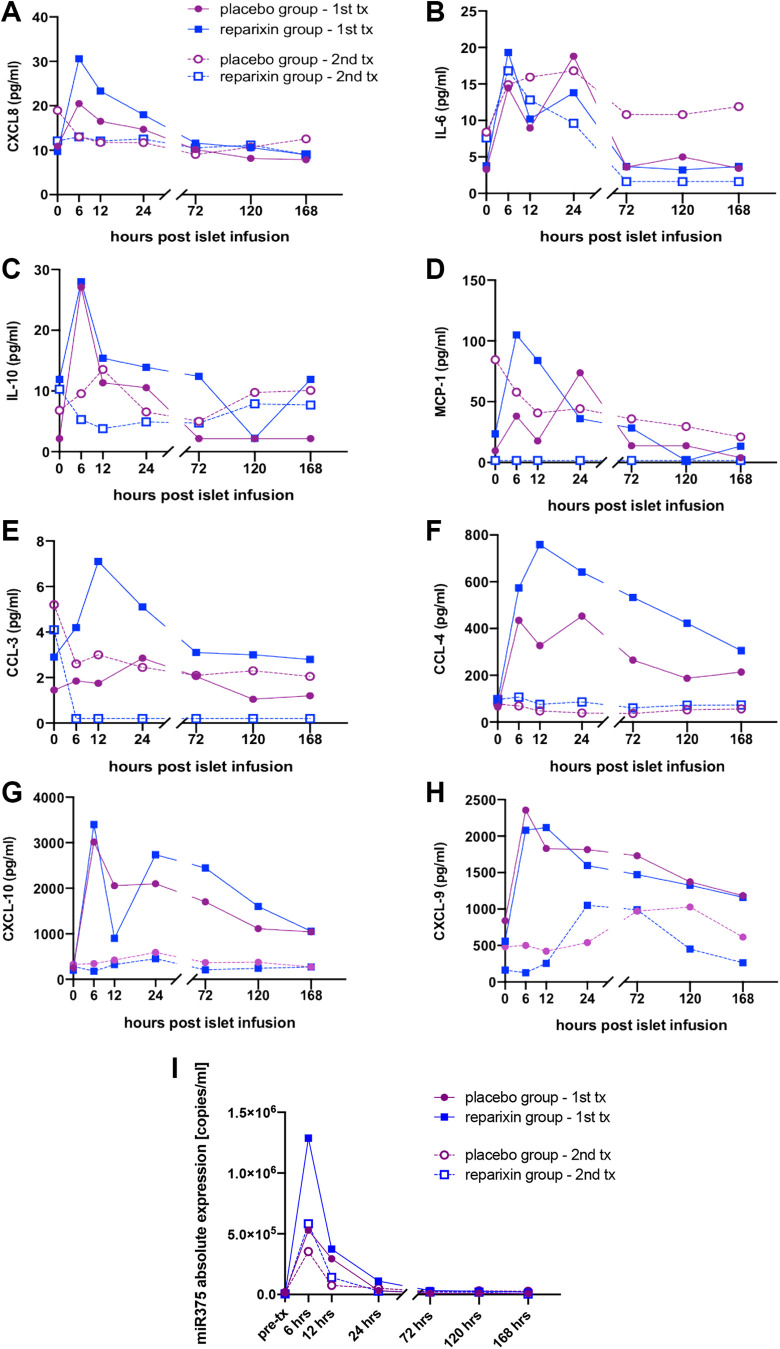
A recent randomized, multicenter trial did not show benefit of a CXCR1/2 receptor inhibitor (Reparixin) when analysis included marginal islet mass (>3,000 IEQ/kg) for allotransplantation and when immunosuppression regimens were not standardized among participating centers. We present a post-hoc analysis of trial patients from our center at the University of Chicago who received an islet mass of over 5,000 IEQ/kg and a standardized immunosuppression regimen of anti-thymocyte globulin (ATG) for induction. Twelve islet allotransplantation (ITx) recipients were randomized (2:1) to receive Reparixin ( = 8) or placebo ( = 4) in accordance with the multicenter trial protocol. Pancreas and donor characteristics did not differ between Reparixin and placebo groups. Five (62.5%) patients who received Reparixin, compared to none in the placebo group, achieved insulin independence after only one islet infusion and remained insulin-free for over 2 years ( = 0.08). Following the first ITx with ATG induction, distinct cytokine, chemokine, and miR-375 release profiles were observed for both the Reparixin and placebo groups. After excluding procedures with complications, islet engraftment on post-operative day 75 after a single transplant was higher in the Reparixin group ( = 7) than in the placebo ( = 3) group ( = 0.03) when islet graft function was measured by the ratio of the area under the curve (AUC) for c-peptide to glucose in mixed meal tolerance test (MMTT). Additionally, the rate of engraftment was higher when determined via BETA-2 score instead of MMTT ( = 0.01). Our analysis suggests that Reparixin may have improved outcomes compared to placebo when sufficient islet mass is transplanted and when standardized immunosuppression with ATG is used for induction. However, further studies are warranted. Investigation of Reparixin and other novel agents under more standardized and optimized conditions would help exclude confounding factors and allow for a more definitive evaluation of their role in improving outcomes in islet transplantation. Clinical trial reg. no. NCT01817959, clinicaltrials.gov.
最近一项随机、多中心试验并未显示 CXCR1/2 受体抑制剂(Reparixin)的益处,当分析包括同种异体移植的边缘胰岛质量(>3000IEQ/kg),并且参与中心之间的免疫抑制方案未标准化时。我们报告了我们在芝加哥大学中心的试验患者的事后分析,这些患者接受了超过 5000IEQ/kg 的胰岛质量,并接受了抗胸腺细胞球蛋白(ATG)的标准化免疫抑制方案进行诱导。根据多中心试验方案,12 名胰岛同种异体移植(ITx)受者被随机(2:1)分为接受 Reparixin(=8)或安慰剂(=4)。Reparixin 和安慰剂组的胰腺和供体特征没有差异。与安慰剂组相比,接受 Reparixin 的 5 名(62.5%)患者在单次胰岛输注后仅实现了胰岛素独立性,并在超过 2 年内保持无胰岛素状态(=0.08)。在首次接受 ATG 诱导的 ITx 后,Reparixin 和安慰剂组均观察到明显的细胞因子、趋化因子和 miR-375 释放谱。在排除有并发症的手术程序后,在单次移植后第 75 天,Reparixin 组(=7)的胰岛移植物植入率高于安慰剂组(=3)(=0.03),当通过混合餐耐量试验(MMTT)中 C 肽与葡萄糖的曲线下面积(AUC)比值来测量胰岛移植物功能时。此外,当通过 BETA-2 评分而不是 MMTT 来确定时,植入率更高(=0.01)。我们的分析表明,当移植足够的胰岛质量并且使用 ATG 进行标准化免疫抑制诱导时,Reparixin 可能比安慰剂更能改善结果。然而,还需要进一步的研究。在更标准化和优化的条件下研究 Reparixin 和其他新型药物将有助于排除混杂因素,并更明确地评估它们在改善胰岛移植结局中的作用。临床试验注册号 NCT01817959,clinicaltrials.gov。