MD. Physician, Department of Urology, Department of Urology, Karabük University Training and Research Hospital, Karabük, Turkey.
MD. Physician, Department of Urology, Health Science University Dr. Abdurrahman Yurtaslan, Ankara Oncology Training and Research Hospital, Ankara, Turkey.
Sao Paulo Med J. 2021 Apr 26;139(3):241-250. doi: 10.1590/1516-3180.2020.0349.R1.28012021. eCollection 2021.
Vesicourethral anastomotic stenosis (VUAS) following retropubic radical prostatectomy (RRP) significantly worsens quality of life.
To investigate the relationship between proliferative hypertrophic scar formation and VUAS, and predict more appropriate surgical intervention for preventing recurrent VUAS.
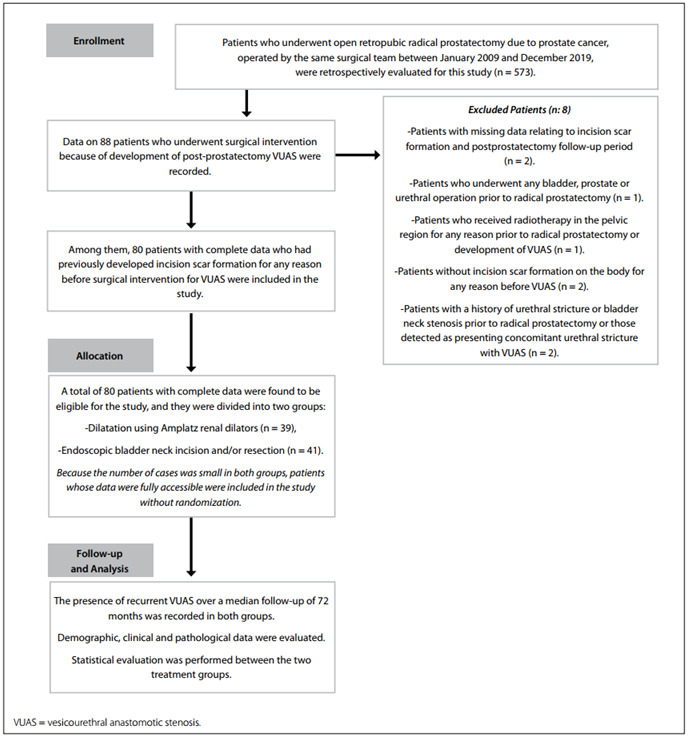
Retrospective cross-sectional single-center study on data covering January 2009 to December 2019.
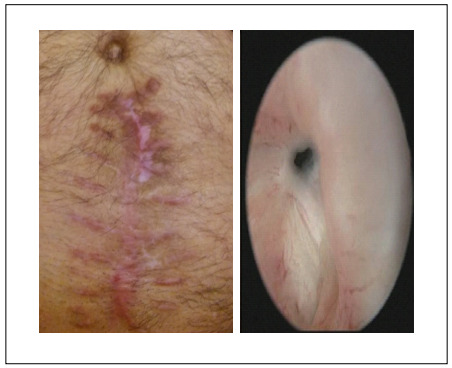
Among 573 male patients who underwent RRP due to prostate cancer, 80 with VUAS were included. They were divided into two groups according to VUAS treatment method: dilatation using Amplatz renal dilators (39 patients); or endoscopic bladder neck incision/resection (41 patients). The Vancouver scar scale (VSS) was used to evaluate the characteristics of scars that occurred for any reason before development of VUAS.
Over a median follow-up of 72 months (range 12-105) after RRP, 17 patients (21.3%) had recurrence of VUAS. Although the treatment success rates were similar (79.5% versus 78.0%; P = 0.875), receiver operating characteristic (ROC) curve analysis indicated that dilatation using Amplatz dilators rather than endoscopic bladder neck incision/resection in patients with VSS scores 4, 5 and 6 may significantly reduce VUAS recurrence. A strong positive relationship was observed between VSS and total number of VUAS occurrences (r: 0.689; P < 0.001). VSS score (odds ratio, OR: 5.380; P < 0.001) and time until occurrence of VUAS (OR: 1.628; P = 0.008) were the most significant predictors for VUAS recurrence.
VSS score can be used as a prediction tool for choosing more appropriate surgical intervention, for preventing recurrent VUAS.
耻骨后前列腺根治性切除术(RRP)后发生的尿道吻合口狭窄(VUAS)显著降低生活质量。
研究增生性肥厚性瘢痕形成与 VUAS 的关系,并预测更合适的手术干预措施以预防 VUAS 复发。
回顾性交叉单中心研究,数据涵盖 2009 年 1 月至 2019 年 12 月。
在因前列腺癌接受 RRP 的 573 名男性患者中,纳入 80 例发生 VUAS 的患者。根据 VUAS 治疗方法将他们分为两组:使用 Amplatz 肾盂扩张器扩张(39 例);或内镜膀胱颈部切开/切除术(41 例)。使用温哥华瘢痕量表(VSS)评估发生 VUAS 之前因任何原因导致的瘢痕特征。
在 RRP 后中位随访 72 个月(范围 12-105)时,17 例(21.3%)患者出现 VUAS 复发。尽管治疗成功率相似(79.5%对 78.0%;P=0.875),但受试者工作特征(ROC)曲线分析表明,对于 VSS 评分为 4、5 和 6 的患者,使用 Amplatz 扩张器而非内镜膀胱颈部切开/切除术进行扩张可能显著降低 VUAS 复发。VSS 与 VUAS 总发生率之间存在强烈的正相关关系(r:0.689;P<0.001)。VSS 评分(优势比,OR:5.380;P<0.001)和发生 VUAS 的时间(OR:1.628;P=0.008)是 VUAS 复发的最显著预测因素。
VSS 评分可作为选择更合适的手术干预措施以预防 VUAS 复发的预测工具。