From the Division of Anesthesiology Critical Care Medicine, Department of Anesthesiology, Center for Health Services Research, and Critical Illness, Brain Dysfunction, and Survivorship Center, Department of Anesthesiology.
Division of Anesthesiology Critical Care Medicine, Department of Anesthesiology, Critical Illness, Brain Dysfunction, and Survivorship Center.
Anesth Analg. 2021 Nov 1;133(5):1152-1161. doi: 10.1213/ANE.0000000000005544.
The temporal association of delirium during critical illness with mortality is unclear, along with the associations of hypoactive and hyperactive motoric subtypes of delirium with mortality. We aimed to evaluate the relationship of delirium during critical illness, including hypoactive and hyperactive motoric subtypes, with mortality in the hospital and after discharge up to 1 year.
We analyzed a prospective cohort study of adults with respiratory failure and/or shock admitted to university, community, and Veterans Affairs hospitals. We assessed patients using the Richmond Agitation-Sedation Scale and the Confusion Assessment Method for the intensive care unit (ICU) and defined the motoric subtype according to the corresponding Richmond Agitation-Sedation Scale if delirium was present. We used Cox proportional hazard models, adjusted for baseline characteristics, coma, and daily hospital events, to determine whether delirium on a given day predicted mortality the following day in patients in the hospital and also to determine whether delirium presence and duration predicted mortality after discharge up to 1 year in patients who survived to hospital discharge. We performed similar analyses for hypoactive and hyperactive subtypes of delirium.
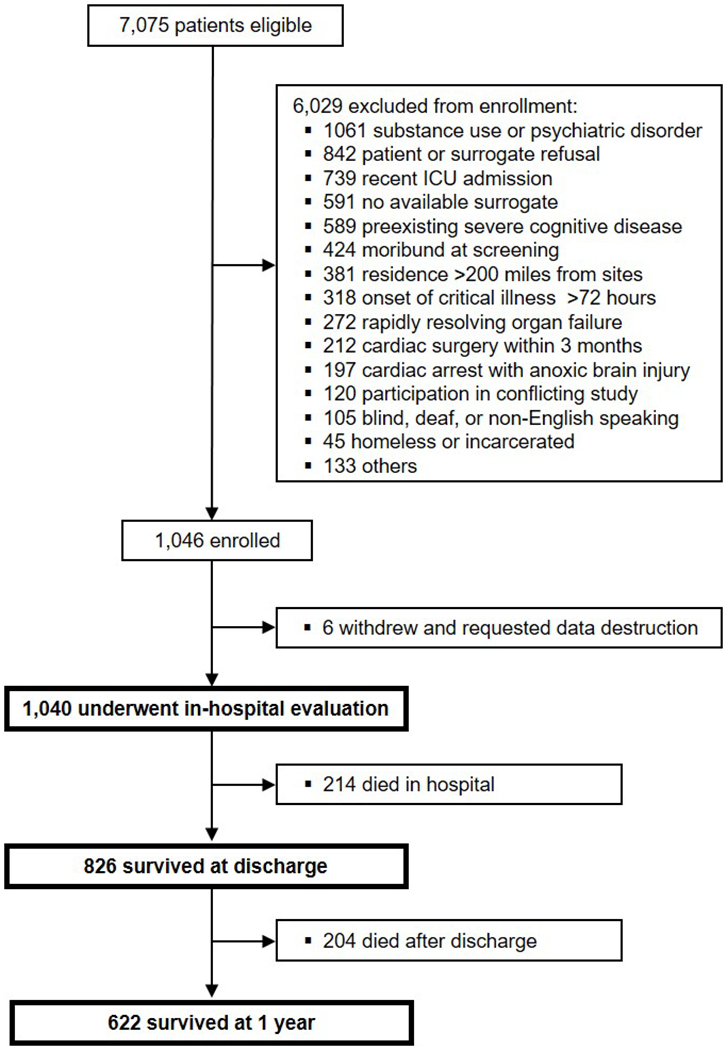
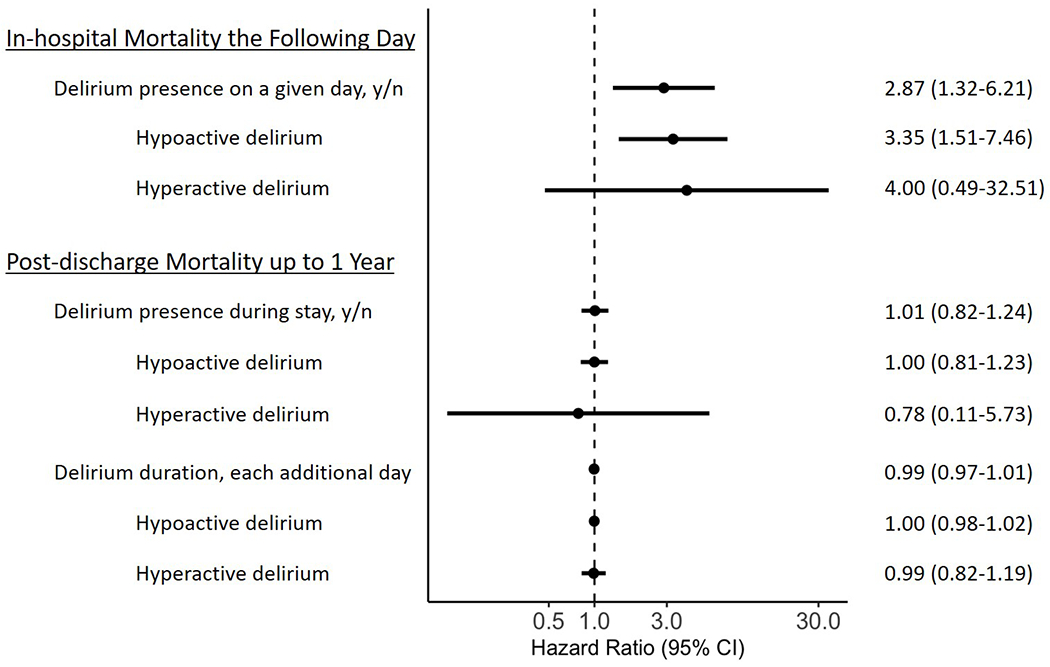
Among 1040 critically ill patients, 214 (21%) died in the hospital and 204 (20%) died out-of-hospital by 1 year. Delirium was common, occurring in 740 (71%) patients for a median (interquartile range [IQR]) of 4 (2-7) days. Hypoactive delirium occurred in 733 (70%) patients, and hyperactive occurred in 185 (18%) patients, with a median (IQR) of 3 (2-7) days and 1 (1-2) days, respectively. Delirium on a given day (hazard ratio [HR], 2.87; 95% confidence interval [CI], 1.32-6.21; P = .008), in particular the hypoactive subtype (HR, 3.35; 95% CI, 1.51-7.46; P = .003), was independently associated with an increased risk of death the following day in the hospital. Hyperactive delirium was not associated with an increased risk of death in the hospital (HR, 4.00; 95% CI, 0.49-32.51; P = .19). Among hospital survivors, neither delirium presence (HR, 1.01; 95% CI, 0.82-1.24; P = .95) nor duration (HR, 0.99; 95% CI, 0.97-1.01; P = .56), regardless of motoric subtype, was associated with mortality after hospital discharge up to 1 year.
Delirium during critical illness is associated with nearly a 3-fold increased risk of death the following day for patients in the hospital but is not associated with mortality after hospital discharge. This finding appears primarily driven by the hypoactive motoric subtype. The independent relationship between delirium and mortality occurs early during critical illness but does not persist after hospital discharge.
在危重病期间,谵妄与死亡率之间的时间关联尚不清楚,而激越型和非激越型运动型谵妄亚型与死亡率之间的关联也是如此。我们旨在评估危重病期间(包括激越型和非激越型运动型谵妄)与院内和出院后 1 年内死亡率之间的关系。
我们分析了一项对患有呼吸衰竭和/或休克的成年患者进行的前瞻性队列研究,这些患者入住了大学、社区和退伍军人事务医院。我们使用 Richmond 激越-镇静量表和 ICU 意识模糊评估法来评估患者,如果存在谵妄,则根据相应的 Richmond 激越-镇静量表来定义运动型亚型。我们使用 Cox 比例风险模型,根据基线特征、昏迷和每日医院事件进行调整,以确定给定日期的谵妄是否会预测次日院内患者的死亡率,以及确定存活至出院的患者出院后 1 年内谵妄的存在和持续时间是否与死亡率相关。我们对激越型和非激越型谵妄亚型进行了类似的分析。
在 1040 名危重症患者中,214 名(21%)在院内死亡,204 名(20%)在出院后 1 年内死亡。谵妄很常见,740 名(71%)患者发生谵妄,中位数(四分位距[IQR])为 4(2-7)天。733 名(70%)患者发生非激越型谵妄,185 名(18%)患者发生激越型谵妄,中位数(IQR)分别为 3(2-7)天和 1(1-2)天。给定日期的谵妄(风险比[HR],2.87;95%置信区间[CI],1.32-6.21;P =.008),特别是非激越型谵妄(HR,3.35;95%CI,1.51-7.46;P =.003),与次日院内死亡风险增加独立相关。激越型谵妄与院内死亡风险增加无关(HR,4.00;95%CI,0.49-32.51;P =.19)。在院内幸存者中,无论是谵妄的存在(HR,1.01;95%CI,0.82-1.24;P =.95)还是持续时间(HR,0.99;95%CI,0.97-1.01;P =.56),都与出院后 1 年内的死亡率无关,无论运动型亚型如何。
在危重病期间发生的谵妄与患者次日的死亡风险增加近 3 倍相关,但与出院后的死亡率无关。这一发现主要归因于非激越型运动型谵妄。谵妄与死亡率之间的独立关系发生在危重病早期,但不会持续到出院后。