Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong Special Administrative Region, China.
Asia Diabetes Foundation, Shatin, Hong Kong Special Administrative Region, China.
JAMA Netw Open. 2021 Apr 1;4(4):e217557. doi: 10.1001/jamanetworkopen.2021.7557.
Many health care systems lack the efficiency, preparedness, or resources needed to address the increasing number of patients with type 2 diabetes, especially in low- and middle-income countries.
To examine the effects of a quality improvement intervention comprising information and communications technology and contact with nonphysician personnel on the care and cardiometabolic risk factors of patients with type 2 diabetes in 8 Asia-Pacific countries.
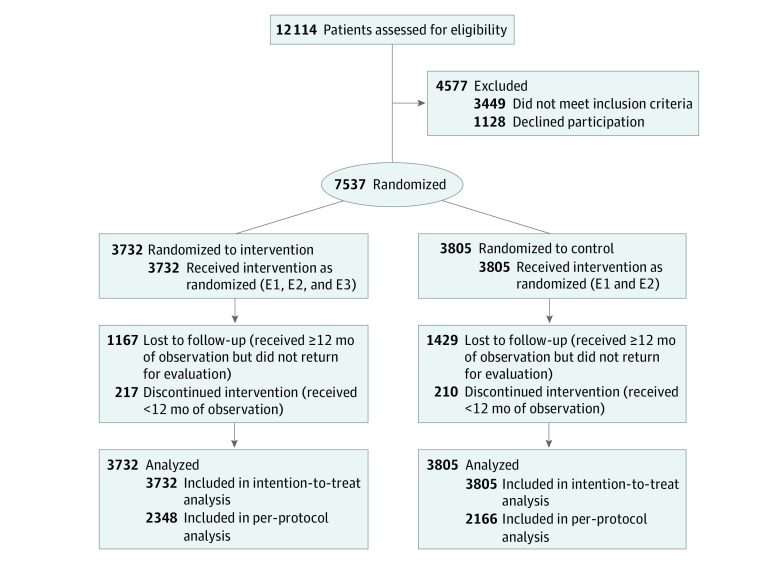
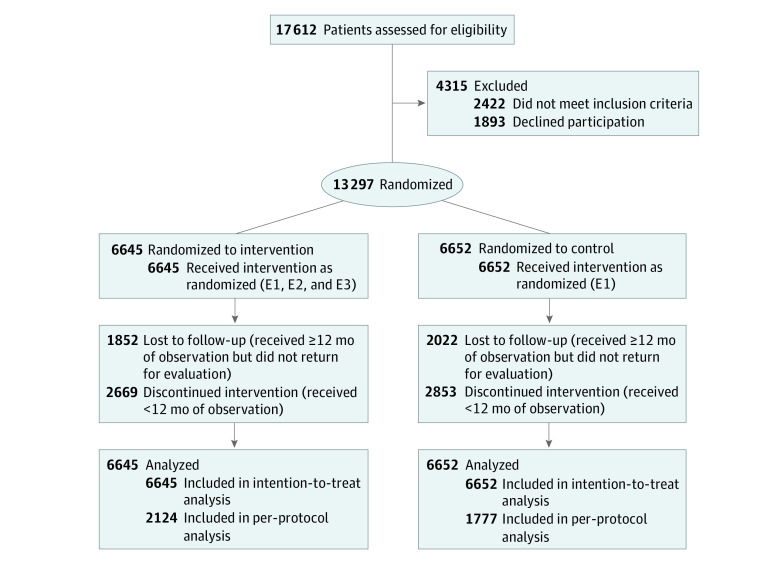
DESIGN, SETTING, AND PARTICIPANTS: This 12-month multinational open-label randomized clinical trial was conducted from June 28, 2012, to April 28, 2016, at 50 primary care or hospital-based diabetes centers in 8 Asia-Pacific countries (India, Indonesia, Malaysia, the Philippines, Singapore, Taiwan, Thailand, and Vietnam). Six countries were low and middle income, and 2 countries were high income. The study was conducted in 2 phases; phase 1 enrolled 7537 participants, and phase 2 enrolled 13 297 participants. Participants in both phases were randomized on a 1:1 ratio to intervention or control groups. Data were analyzed by intention to treat and per protocol from July 3, 2019, to July 21, 2020.
In both phases, the intervention group received 3 care components: a nurse-led Joint Asia Diabetes Evaluation (JADE) technology-guided structured evaluation, automated personalized reports to encourage patient empowerment, and 2 or more telephone or face-to-face contacts by nurses to increase patient engagement. In phase 1, the control group received the JADE technology-guided structured evaluation and automated personalized reports. In phase 2, the control group received the JADE technology-guided structured evaluation only.
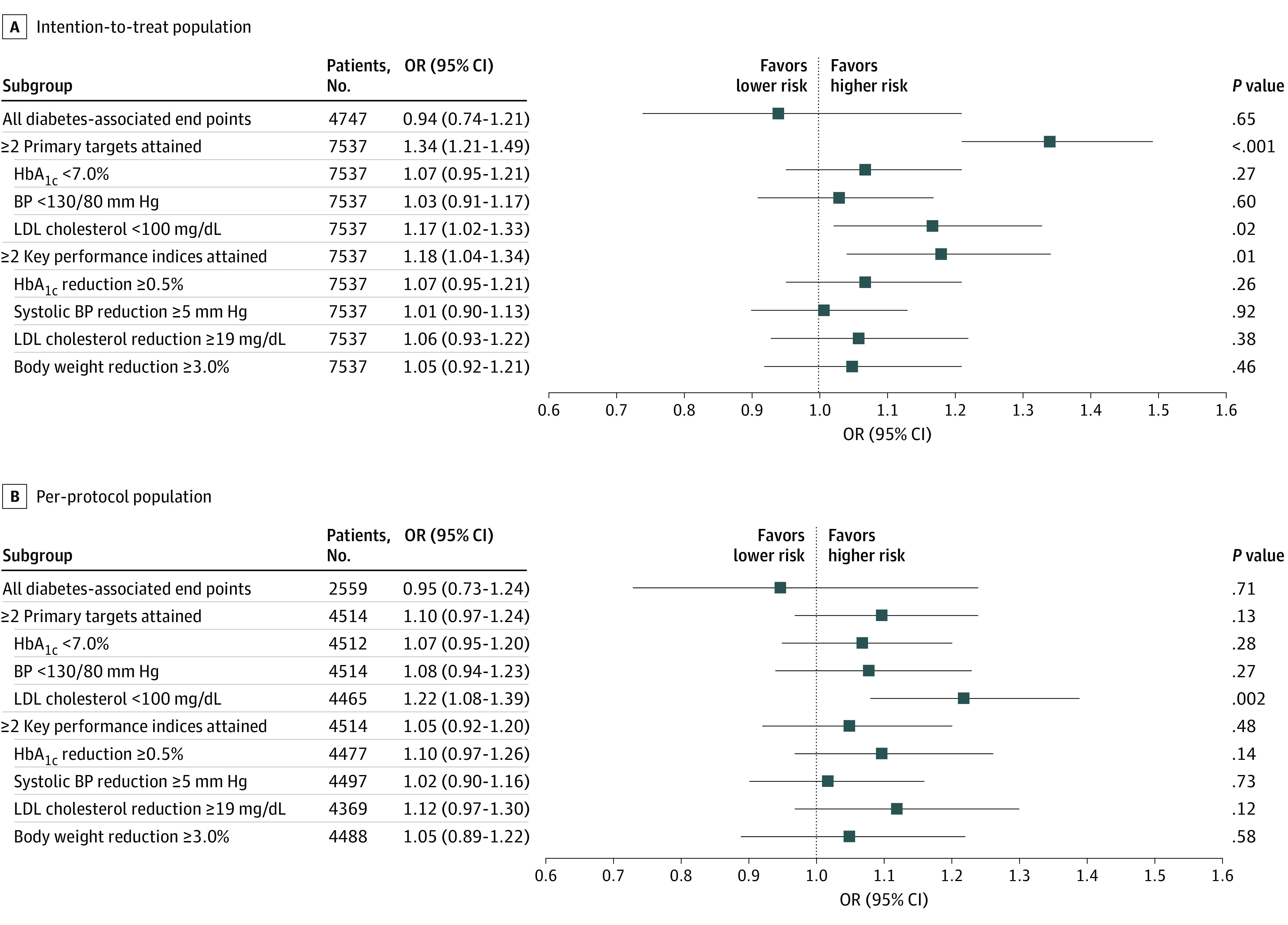
The primary outcome was the incidence of a composite of diabetes-associated end points, including cardiovascular disease, chronic kidney disease, visual impairment or eye surgery, lower extremity amputation or foot ulcers requiring hospitalization, all-site cancers, and death. The secondary outcomes were the attainment of 2 or more primary diabetes-associated targets (glycated hemoglobin A1c <7.0%, blood pressure <130/80 mm Hg, and low-density lipoprotein cholesterol <100 mg/dL) and/or 2 or more key performance indices (reduction in glycated hemoglobin A1c≥0.5%, reduction in systolic blood pressure ≥5 mm Hg, reduction in low-density lipoprotein cholesterol ≥19 mg/dL, and reduction in body weight ≥3.0%).
A total of 20 834 patients with type 2 diabetes were randomized in phases 1 and 2. In phase 1, 7537 participants (mean [SD] age, 60.0 [11.3] years; 3914 men [51.9%]; 4855 patients [64.4%] from low- and middle-income countries) were randomized, with 3732 patients allocated to the intervention group and 3805 patients allocated to the control group. In phase 2, 13 297 participants (mean [SD] age, 54.0 [11.1] years; 7754 men [58.3%]; 13 297 patients [100%] from low- and middle-income countries) were randomized, with 6645 patients allocated to the intervention group and 6652 patients allocated to the control group. In phase 1, compared with the control group, the intervention group had a similar risk of experiencing any of the primary outcomes (odds ratio [OR], 0.94; 95% CI, 0.74-1.21) but had an increased likelihood of attaining 2 or more primary targets (OR, 1.34; 95% CI, 1.21-1.49) and 2 or more key performance indices (OR, 1.18; 95% CI, 1.04-1.34). In phase 2, the intervention group also had a similar risk of experiencing any of the primary outcomes (OR, 1.02; 95% CI, 0.83-1.25) and had a greater likelihood of attaining 2 or more primary targets (OR, 1.25; 95% CI, 1.14-1.37) and 2 or more key performance indices (OR, 1.50; 95% CI, 1.33-1.68) compared with the control group. For attainment of 2 or more primary targets, larger effects were observed among patients in low- and middle-income countries (OR, 1.50; 95% CI, 1.29-1.74) compared with high-income countries (OR, 1.20; 95% CI, 1.03-1.39) (P = .04).
In this 12-month clinical trial, the use of information and communications technology and nurses to empower and engage patients did not change the number of clinical events but did reduce cardiometabolic risk factors among patients with type 2 diabetes, especially those in low- and middle-income countries in the Asia-Pacific region.
ClinicalTrials.gov Identifier: NCT01631084.
许多医疗保健系统缺乏应对不断增加的 2 型糖尿病患者所需的效率、准备和资源,尤其是在低收入和中等收入国家。
研究由信息和通信技术以及与非医师人员联系组成的质量改进干预措施对 8 个亚太国家的 2 型糖尿病患者的护理和心血管代谢风险因素的影响。
设计、设置和参与者:这项为期 12 个月的多国开放标签随机临床试验于 2012 年 6 月 28 日至 2016 年 4 月 28 日在 8 个亚太国家(印度、印度尼西亚、马来西亚、菲律宾、新加坡、中国台湾、泰国和越南)的 50 个初级保健或医院为基础的糖尿病中心进行。其中 6 个国家为中低收入国家,2 个国家为高收入国家。该研究分 2 个阶段进行;第 1 阶段纳入 7537 名参与者,第 2 阶段纳入 13297 名参与者。两个阶段的参与者均按 1:1 的比例随机分配至干预组或对照组。数据分析于 2019 年 7 月 3 日至 2020 年 7 月 21 日按意向治疗和方案进行。
在两个阶段中,干预组都接受了 3 个护理组件:护士主导的联合亚洲糖尿病评估(JADE)技术指导的结构化评估、鼓励患者授权的自动化个性化报告以及增加患者参与度的 2 次或更多次电话或面对面的护士接触。在第 1 阶段,对照组接受 JADE 技术指导的结构化评估和自动化个性化报告。在第 2 阶段,对照组仅接受 JADE 技术指导的结构化评估。
主要结局是包括心血管疾病、慢性肾脏病、视力损害或眼部手术、下肢截肢或需要住院治疗的足部溃疡、所有部位癌症和死亡在内的糖尿病相关终点的复合发生率。次要结局是达到 2 个或更多主要糖尿病相关目标(糖化血红蛋白 A1c<7.0%、血压<130/80mmHg 和低密度脂蛋白胆固醇<100mg/dL)和/或 2 个或更多关键绩效指标(糖化血红蛋白 A1c 降低≥0.5%、收缩压降低≥5mmHg、低密度脂蛋白胆固醇降低≥19mg/dL 和体重减轻≥3.0%)。
共有 20834 名 2 型糖尿病患者被随机分配至第 1 阶段和第 2 阶段。在第 1 阶段,7537 名参与者(平均[SD]年龄 60.0[11.3]岁;3914 名男性[51.9%];4855 名患者[64.4%]来自中低收入国家)被随机分组,3732 名参与者被分配至干预组,3805 名参与者被分配至对照组。在第 2 阶段,13297 名参与者(平均[SD]年龄 54.0[11.1]岁;7754 名男性[58.3%];13297 名患者[100%]来自中低收入国家)被随机分组,6645 名参与者被分配至干预组,6652 名参与者被分配至对照组。在第 1 阶段,与对照组相比,干预组发生任何主要结局的风险相似(比值比[OR],0.94;95%置信区间[CI],0.74-1.21),但更有可能达到 2 个或更多主要目标(OR,1.34;95%CI,1.21-1.49)和 2 个或更多关键绩效指标(OR,1.18;95%CI,1.04-1.34)。在第 2 阶段,干预组发生任何主要结局的风险也相似(OR,1.02;95%CI,0.83-1.25),且达到 2 个或更多主要目标(OR,1.25;95%CI,1.14-1.37)和 2 个或更多关键绩效指标(OR,1.50;95%CI,1.33-1.68)的可能性更大,与对照组相比。对于达到 2 个或更多主要目标,中低收入国家的患者观察到的效果更大(OR,1.50;95%CI,1.29-1.74),而高收入国家的患者(OR,1.20;95%CI,1.03-1.39)(P=0.04)。
在这项为期 12 个月的临床试验中,使用信息和通信技术以及护士来赋予和吸引患者的能力并没有改变临床事件的数量,但确实降低了 2 型糖尿病患者的心血管代谢风险因素,尤其是在亚太地区的中低收入国家。
ClinicalTrials.gov 标识符:NCT01631084。