Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong SAR, China.
Asia Diabetes Foundation, Shatin, Hong Kong SAR, China.
PLoS Med. 2020 Oct 2;17(10):e1003367. doi: 10.1371/journal.pmed.1003367. eCollection 2020 Oct.
Diabetes outcomes are influenced by host factors, settings, and care processes. We examined the association of data-driven integrated care assisted by information and communications technology (ICT) with clinical outcomes in type 2 diabetes in public and private healthcare settings.
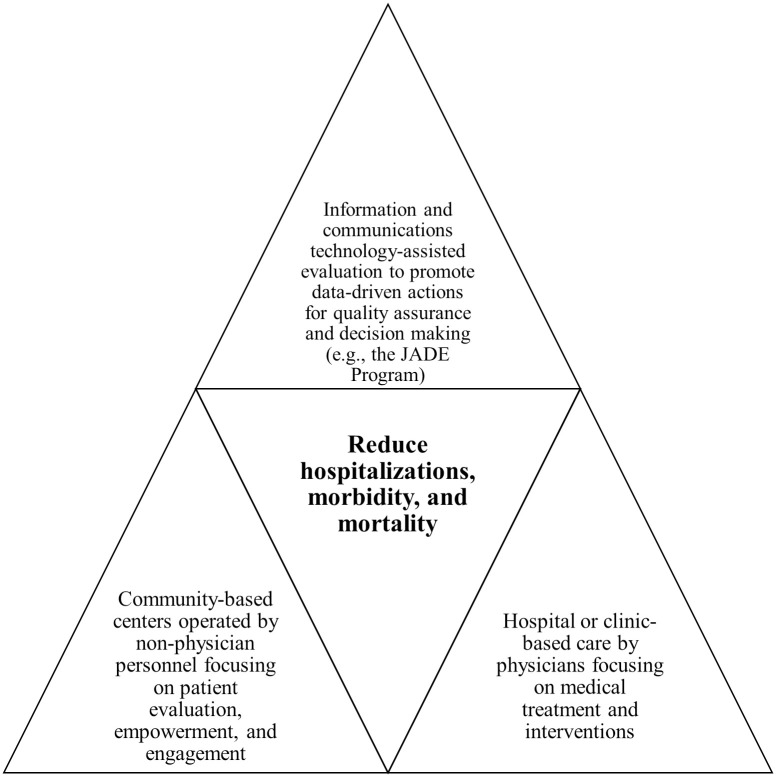
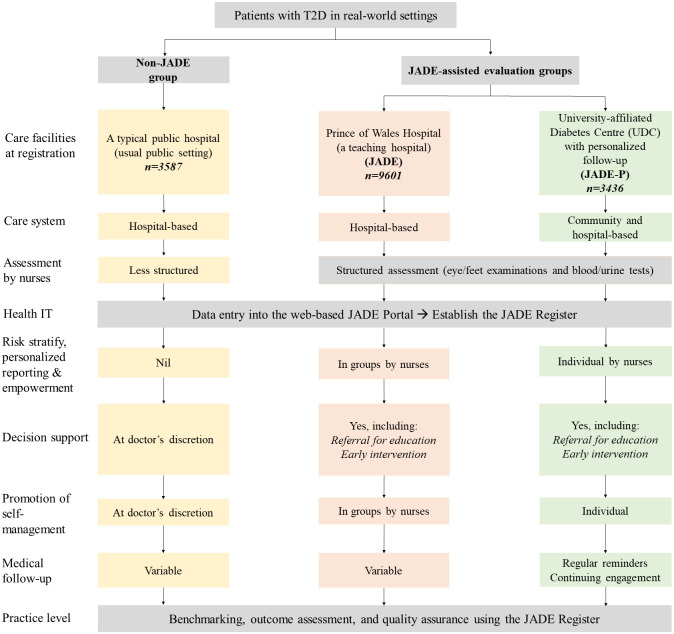
The web-based Joint Asia Diabetes Evaluation (JADE) platform provides a protocol to guide data collection for issuing a personalized JADE report including risk categories (1-4, low-high), 5-year probabilities of cardiovascular-renal events, and trends and targets of 4 risk factors with tailored decision support. The JADE program is a prospective cohort study implemented in a naturalistic environment where patients underwent nurse-led structured evaluation (blood/urine/eye/feet) in public and private outpatient clinics and diabetes centers in Hong Kong. We retrospectively analyzed the data of 16,624 Han Chinese patients with type 2 diabetes who were enrolled in 2007-2015. In the public setting, the non-JADE group (n = 3,587) underwent structured evaluation for risk factors and complications only, while the JADE (n = 9,601) group received a JADE report with group empowerment by nurses. In a community-based, nurse-led, university-affiliated diabetes center (UDC), the JADE-Personalized (JADE-P) group (n = 3,436) received a JADE report, personalized empowerment, and annual telephone reminder for reevaluation and engagement. The primary composite outcome was time to the first occurrence of cardiovascular-renal diseases, all-site cancer, and/or death, based on hospitalization data censored on 30 June 2017. During 94,311 person-years of follow-up in 2007-2017, 7,779 primary events occurred. Compared with the JADE group (136.22 cases per 1,000 patient-years [95% CI 132.35-140.18]), the non-JADE group had higher (145.32 [95% CI 138.68-152.20]; P = 0.020) while the JADE-P group had lower event rates (70.94 [95% CI 67.12-74.91]; P < 0.001). The adjusted hazard ratios (aHRs) for the primary composite outcome were 1.22 (95% CI 1.15-1.30) and 0.70 (95% CI 0.66-0.75), respectively, independent of risk profiles, education levels, drug usage, self-care, and comorbidities at baseline. We reported consistent results in propensity-score-matched analyses and after accounting for loss to follow-up. Potential limitations include its nonrandomized design that precludes causal inference, residual confounding, and participation bias.
ICT-assisted integrated care was associated with a reduction in clinical events, including death in type 2 diabetes in public and private healthcare settings.
糖尿病的结果受到宿主因素、环境和护理过程的影响。我们研究了在公共和私人医疗保健环境中,由信息和通信技术(ICT)辅助的数据驱动的综合护理与 2 型糖尿病临床结果之间的关联。
基于网络的联合亚洲糖尿病评估(JADE)平台提供了一个方案,用于指导数据收集,以发布个性化的 JADE 报告,包括风险类别(1-4,低-高)、5 年内心血管-肾脏事件的概率,以及 4 个风险因素的趋势和目标,同时提供量身定制的决策支持。JADE 项目是一项前瞻性队列研究,在自然环境中实施,患者在香港的公共和私人门诊诊所和糖尿病中心接受护士主导的结构化评估(血液/尿液/眼睛/脚部)。我们回顾性分析了 2007 年至 2015 年期间纳入的 16624 名汉族 2 型糖尿病患者的数据。在公共环境中,非 JADE 组(n=3587)仅接受风险因素和并发症的结构化评估,而 JADE 组(n=9601)则接受了护士组授权的 JADE 报告。在以社区为基础、护士主导、与大学相关的糖尿病中心(UDC)中,JADE-个性化(JADE-P)组(n=3436)接受了 JADE 报告、个性化授权和每年的电话提醒,以重新评估和参与。主要复合结局是首次发生心血管-肾脏疾病、所有部位癌症和/或死亡的时间,根据 2017 年 6 月 30 日的住院数据进行 censored。在 2007 年至 2017 年的 94311 人年随访中,发生了 7779 例主要事件。与 JADE 组(每 1000 名患者年 136.22 例[95%CI 132.35-140.18])相比,非 JADE 组的发生率更高(145.32[95%CI 138.68-152.20];P=0.020),而 JADE-P 组的发生率较低(70.94[95%CI 67.12-74.91];P<0.001)。主要复合结局的调整后的危害比(aHR)分别为 1.22(95%CI 1.15-1.30)和 0.70(95%CI 0.66-0.75),独立于基线时的风险状况、教育程度、药物使用、自我护理和合并症。在倾向评分匹配分析和考虑失随访后,我们报告了一致的结果。潜在的局限性包括其非随机设计,这妨碍了因果推断、残余混杂和参与偏倚。
在公共和私人医疗保健环境中,由信息和通信技术辅助的综合护理与 2 型糖尿病的临床事件减少相关,包括死亡。