Department of Obstetrics and Gynecology, Peking University Shenzhen Hospital, 1120 Lianhua Road, Shenzhen, Guangdong, 518036, P. R. China.
Institute of Obstetrics and Gynecology, Shenzhen PKU-HKUST Medical Center, Shenzhen, Guangdong, 518036, P. R. China.
BMC Infect Dis. 2021 Apr 30;21(1):400. doi: 10.1186/s12879-021-06109-4.
Self-sampling for human papillomavirus (HPV) testing is a feasible option to improve the cervical screening coverage. However, an ideal triage method for HPV-positive self-samples does not yet exist. The aim of this study was to explore the utility of HPV genotyping and p16 immunostaining (p16) in triaging HPV-positive self-samples, focusing on HPV-positive, cytology-negative (HPCN) women.
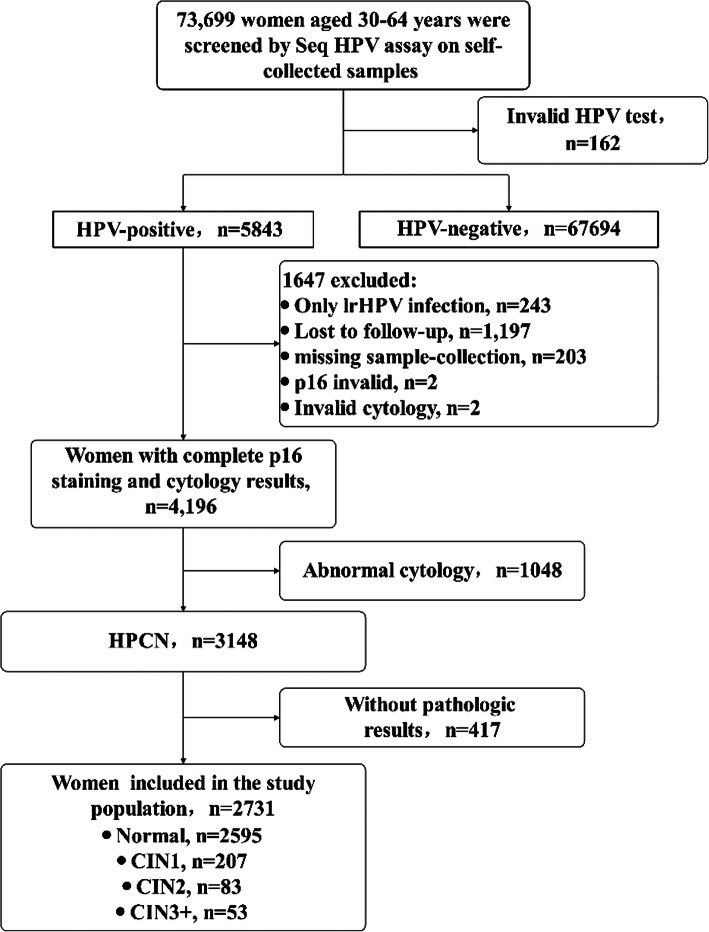
A total of 73,699 women were screened in a cervical screening project in China via SeqHPV assay on self-samples. HPV-positive women were called-back and collected cervical sample for p16 immunostaining and liquid-based cytology, those who met any result of HPV16/18+ or visual inspection with acetic acid (VIA) + or p16+ were referred for colposcopy, and HPCN women with adequate data on p16 and pathology were analyzed. A triage strategy was considered acceptable if the negative predictive value (NPV) for cervical intraepithelial neoplasia 3 or worse (CIN3+) was 98% or more, combined with an improvement of sensitivity and specificity for CIN2+/CIN3+ in reference to the comparator, being HPV16/18 + .
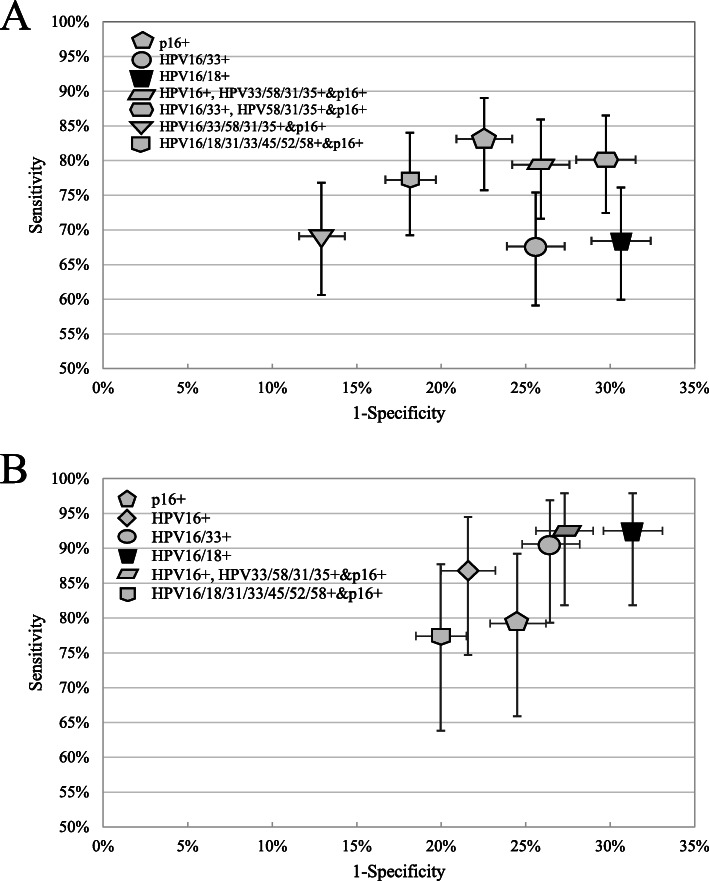
A total of 2731 HPCN women aged 30-64 years were enrolled, 136 (5.0%) CIN2+ and 53 (1.9%) CIN3+ were detected. Five triage strategies met the criteria: p16+; HPV16/33+; 'HPV16+ or HPV33/58/31/35+&p16+'; 'HPV16/33+ or HPV58/31/35+&p16+'; HPV16/18/31/33/45/52/58 + & p16+. These strategies required less or similar colposcopy referrals, and less colposcopies to detected one case of CIN2+/CIN3+, achieving favorable false positive (negative) rates to the comparator. Among them, p16 staining detected 83.1% (79.2%) of underlying CIN2 + (CIN3+) in HPCN women. Moreover, three triage strategies were favorable in sensitivity and/or specificity to the 'HPV16/33+' strategy: p16+; 'HPV16+ or HPV33/58/31/35 + &p16+'; HPV16/18/31/33/45/52/58 + &p16 + .
Genotyping for HPV16/33 could be utilized to optimize the management of HPCN women. Moreover, p16 immunostaining, either alone or combined with extended genotypes, is more effective than HPV genotypes alone in the triage of HPCN women.
人乳头瘤病毒(HPV)自我采样检测是提高宫颈筛查覆盖率的可行选择。然而,HPV 阳性自我样本的理想分流方法尚未存在。本研究旨在探索 HPV 基因分型和 p16 免疫染色(p16)在 HPV 阳性自我样本分流中的效用,重点关注 HPV 阳性、细胞学阴性(HPCN)女性。
在中国的一项宫颈筛查项目中,共有 73699 名妇女通过自我样本上的 SeqHPV 检测进行筛查。HPV 阳性的妇女被召回,并采集宫颈样本进行 p16 免疫染色和液基细胞学检查,符合 HPV16/18+或醋酸视觉检查(VIA)+或 p16+结果的妇女被转诊行阴道镜检查,对具有足够 p16 和病理数据的 HPCN 妇女进行分析。如果用于 CIN3+的阴性预测值(NPV)为 98%或更高,并且与比较组相比,对 CIN2+/CIN3+的敏感性和特异性有所提高,同时将 HPV16/18+作为参考,则认为分流策略是可接受的。
共纳入 2731 名年龄在 30-64 岁的 HPCN 妇女,检出 136 例 CIN2+和 53 例 CIN3+。五种分流策略符合标准:p16+;HPV16/33+;“HPV16+或 HPV33/58/31/35+&p16+”;“HPV16/33+或 HPV58/31/35+&p16+”;HPV16/18/31/33/45/52/58+&p16+。这些策略需要较少或类似的阴道镜转诊,并且需要较少的阴道镜检查来检测到一个 CIN2+/CIN3+病例,达到了对比较组有利的假阳性(阴性)率。其中,p16 染色在 HPCN 妇女中检测到 83.1%(79.2%)的潜在 CIN2+(CIN3+)。此外,三种分流策略在敏感性和/或特异性方面优于“HPV16/33+”策略:p16+;“HPV16+或 HPV33/58/31/35+&p16+”;HPV16/18/31/33/45/52/58+&p16+。
HPV16/33 的基因分型可用于优化 HPCN 妇女的管理。此外,p16 免疫染色,单独使用或与扩展的基因型联合使用,在 HPCN 妇女的分流中比 HPV 基因型单独使用更有效。