Department of Otolaryngology-Head and Neck Surgery, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Department of Radiation Oncology, The University of North Carolina at Chapel Hill, Chapel Hill, NC, USA.
Cancer Med. 2021 May;10(10):3231-3239. doi: 10.1002/cam4.3883. Epub 2021 May 2.
Only high-risk tumors with extranodal extension (ENE) and/or positive surgical margins (PSM) benefit from adjuvant therapy (AT) with concurrent chemoradiation (CRT) compared to radiation therapy (RT) in locally advanced head and neck squamous cell carcinoma (HNSCC). Optimal treatment for intermediate-risk tumors remains controversial. We categorized patients based on their surgical pathologic risk factors and described AT treatment patterns and associated survival outcomes.
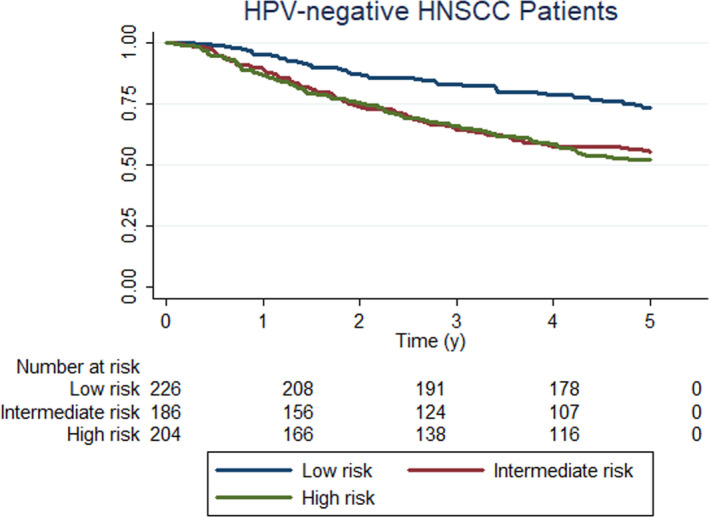
Patients were identified from CHANCE, a population-based study, and risk was classified based on surgical pathology review. High-risk patients (n = 204) required ENE and/or PSM. Intermediate-risk (n = 186) patients had pathological T3/T4 disease, perineural invasion (PNI), lymphovascular invasion (LVI), or positive lymph nodes without ENE. Low-risk patients (n = 226) had none of these features.
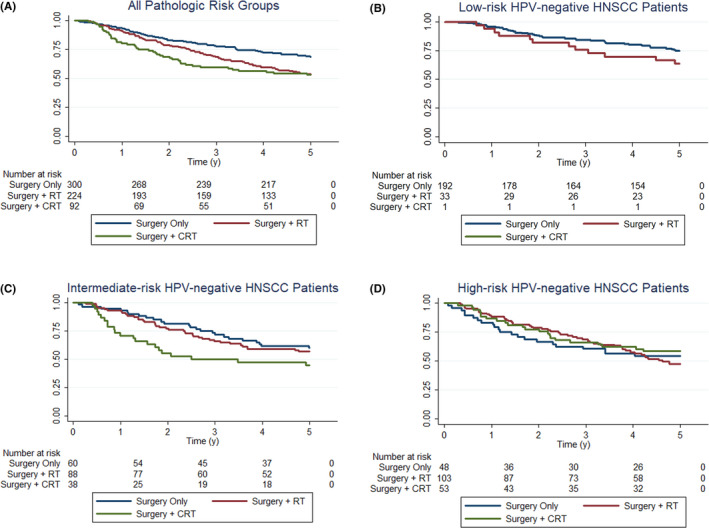
We identified 616 HPV-negative HNSCC patients who received primary surgical resection with neck dissection. High-risk patients receiving AT had favorable OS (HR 0.50, p = 0.013) which was significantly improved with the addition of chemotherapy compared to RT alone (HR 0.47, p = 0.021). When stratified by node status, the survival benefit of AT in high-risk patients persisted only among those who were node-positive (HR: 0.17, p < 0.0005). On the contrary, intermediate-risk patients did not benefit from AT (HR: 1.26, p = 0.380) and the addition of chemotherapy was associated with significantly worse OS compared to RT (HR: 1.76, p = 0.046).
In high-risk patients, adjuvant chemoradiotherapy improved OS compared to RT alone. The greatest benefit was in node-positive cases. In intermediate-risk patients, the addition of chemotherapy to RT increased mortality risk and therefore should only be used cautiously in these patients.
在局部晚期头颈部鳞状细胞癌(HNSCC)中,只有具有结外侵犯(ENE)和/或阳性手术切缘(PSM)的高危肿瘤从辅助治疗(AT)与同期放化疗(CRT)中获益,而不是放射治疗(RT)。对于中危肿瘤的最佳治疗仍存在争议。我们根据手术病理危险因素对患者进行分类,并描述了 AT 治疗模式和相关的生存结果。
从基于人群的 CHANCE 研究中确定患者,并根据手术病理复查进行风险分类。高危患者(n=204)需要有 ENE 和/或 PSM。中危(n=186)患者具有病理性 T3/T4 疾病、神经周围侵犯(PNI)、血管淋巴管侵犯(LVI)或无 ENE 的阳性淋巴结。低危患者(n=226)没有这些特征。
我们确定了 616 例接受原发手术切除和颈部清扫术的 HPV 阴性 HNSCC 患者。接受 AT 的高危患者具有良好的 OS(HR 0.50,p=0.013),与单独接受 RT 相比,添加化疗显著改善(HR 0.47,p=0.021)。按淋巴结状态分层时,AT 在高危患者中的生存获益仅在淋巴结阳性患者中持续(HR:0.17,p<0.0005)。相反,中危患者不能从 AT 中获益(HR:1.26,p=0.380),并且添加化疗与 RT 相比显著降低 OS(HR:1.76,p=0.046)。
在高危患者中,辅助放化疗与单独 RT 相比改善了 OS。最大获益见于淋巴结阳性病例。在中危患者中,RT 中添加化疗增加了死亡风险,因此在这些患者中应谨慎使用。