Department of Pediatrics, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Department of Haematology, Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India.
Front Immunol. 2021 Apr 16;12:627651. doi: 10.3389/fimmu.2021.627651. eCollection 2021.
Wiskott Aldrich syndrome (WAS) is characterized by bleeding manifestations, recurrent infections, eczema, autoimmunity, and malignancy. Over the last decade, improved awareness and better in-house diagnostic facilities at several centers in India has resulted in increased recognition of WAS. This study reports collated data across major primary immunodeficiency diseases (PID) centers in India that are involved in care of children with WAS and highlights the varied clinical presentations, genetic profile, and outcomes of patients in India.
Request to share data was sent to multiple centers in India that are involved in care and management of patients with PID. Six centers provided requisite data that were compiled and analyzed.
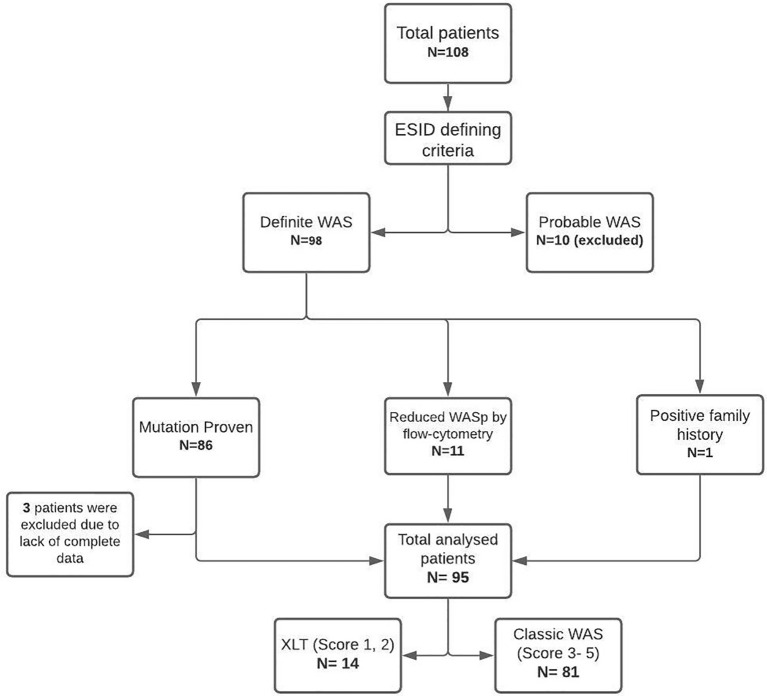
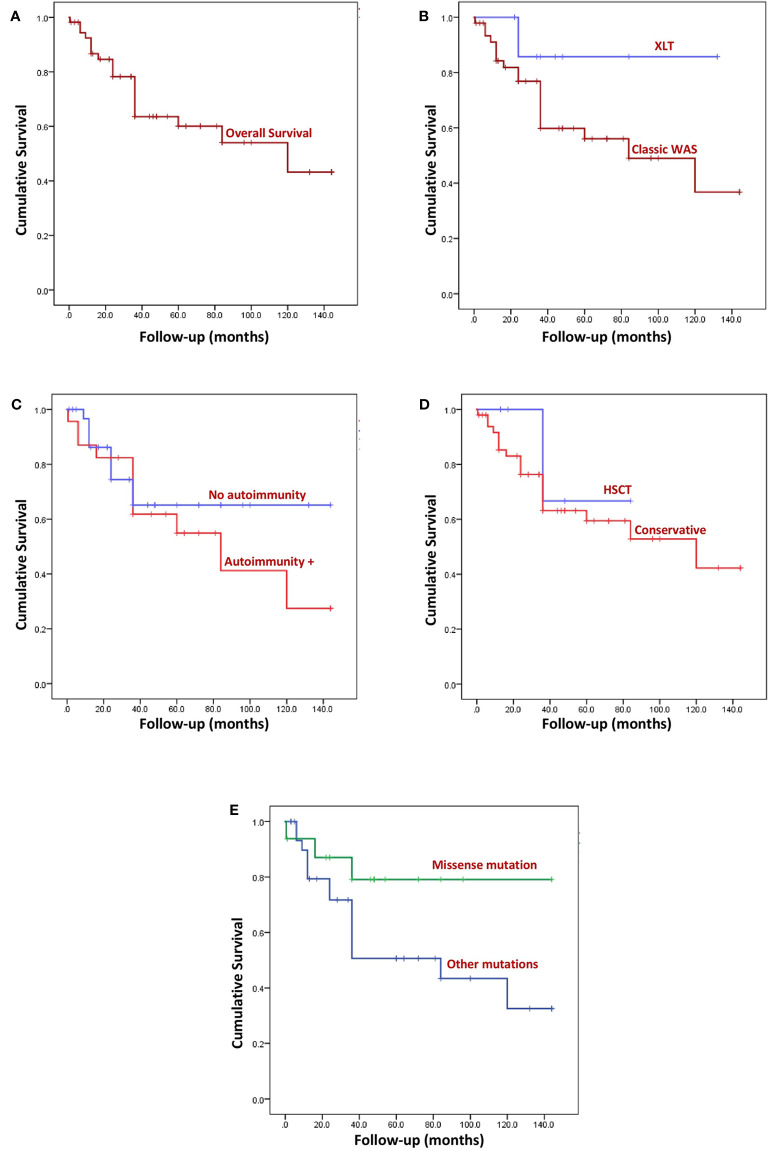
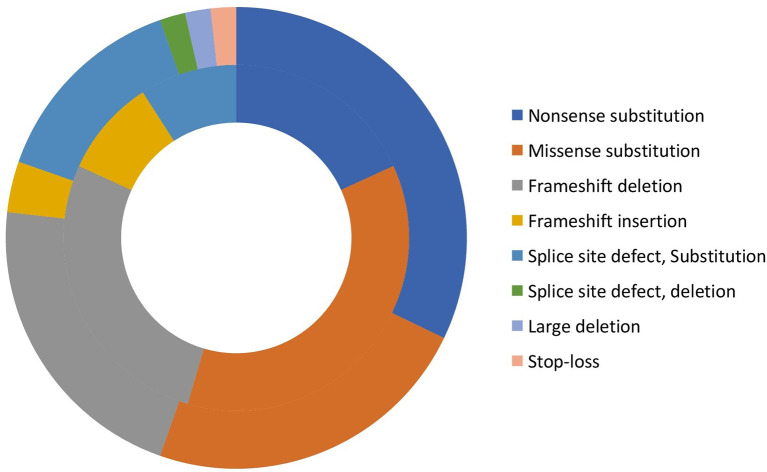
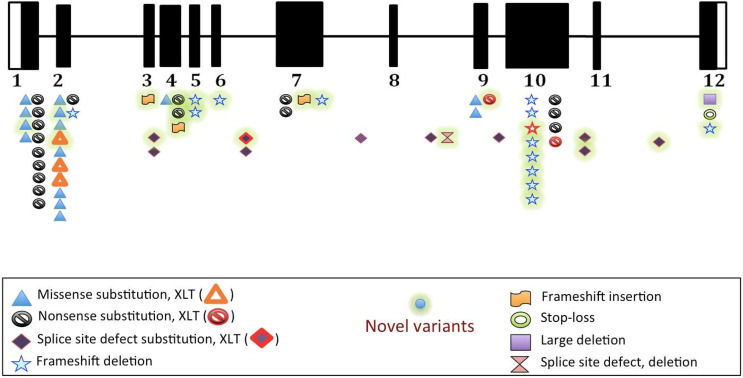
In this multi-institutional cohort, clinical details of 108 patients who had a provisional diagnosis of WAS were received. Of these, 95 patients with 'definite WAS' were included Fourteen patients were classified as XLT and 81 patients as WAS. Median age at onset of symptoms of patients was 3 months (IQR 1.6, 6.0 months) and median age at diagnosis was 12 months (IQR 6,48 months). Clinical profile included bleeding episodes (92.6%), infections (84.2%), eczema (78.9%), various autoimmune manifestations (40%), and malignancy (2.1%). DNA analysis revealed 47 variants in 67 cases. Nonsense and missense variants were the most common (28.4% each), followed by small deletions (19.4%), and splice site defects (16.4%). We also report 24 novel variants, most of these being frameshift and nonsense mutations resulting in premature termination of protein synthesis. Prophylactic intravenous immunoglobulin (IVIg) was initiated in 52 patients (54.7%). Hematopoietic stem cell transplantation (HSCT) was carried out in 25 patients (26.3%). Of those transplanted, disease-free survival was seen in 15 patients (60%). Transplant related mortality was 36%. Outcome details were available for 89 patients. Of these, 37% had died till the time of this analysis. Median duration of follow-up was 36 months (range 2 weeks- 12 years; IQR 16.2 months- 70 months).
We report the first nationwide cohort of patients with WAS from India. Bleeding episodes and infections are common manifestations. Mortality continues to be high as curative therapy is not accessible to most of our patients.
Wiskott-Aldrich 综合征(WAS)的特征是出血表现、反复感染、湿疹、自身免疫和恶性肿瘤。在过去的十年中,印度的几个中心提高了认识,并改善了内部诊断设施,这导致了 WAS 的发病率增加。本研究报告了印度多个主要原发性免疫缺陷病(PID)中心对 WAS 患儿进行护理的汇总数据,并强调了印度患者的不同临床表现、基因谱和预后。
向参与 PID 患儿治疗和管理的印度多个中心发送了分享数据的请求。六个中心提供了必要的数据,这些数据被汇编和分析。
在这个多机构队列中,收到了 108 名疑似 WAS 患者的临床详细信息。其中,95 名“明确的 WAS”患者被纳入研究。14 名患者被归类为 XLT,81 名患者被归类为 WAS。患者症状出现的中位年龄为 3 个月(IQR 1.6,6.0 个月),诊断时的中位年龄为 12 个月(IQR 6,48 个月)。临床特征包括出血发作(92.6%)、感染(84.2%)、湿疹(78.9%)、各种自身免疫表现(40%)和恶性肿瘤(2.1%)。DNA 分析显示在 67 例中发现了 47 种变异。无意义和错义变异最常见(各占 28.4%),其次是小缺失(19.4%)和剪接位点缺陷(16.4%)。我们还报告了 24 种新的变异,其中大多数是移码和无意义突变,导致蛋白质合成过早终止。52 名患者(54.7%)开始预防性静脉注射免疫球蛋白(IVIg)。25 名患者(26.3%)接受了造血干细胞移植(HSCT)。在接受移植的患者中,15 名(60%)患者无疾病生存。移植相关死亡率为 36%。89 名患者的预后详情可获得。其中,37%的患者在分析时已经死亡。中位随访时间为 36 个月(范围 2 周-12 年;IQR 16.2 个月-70 个月)。
我们报告了印度首例全国性 WAS 患者队列。出血发作和感染是常见的表现。由于大多数患者无法获得根治性治疗,死亡率仍然很高。