Quesada Odayme, Shandhi Md Mobashir Hasan, Beach Shire, Dowling Sean, Tandon Damini, Heller James, Etemadi Mozziyar, Roy Shuvo, Gonzalez Velez Juan M, Inan Omer T, Klein Liviu
Women's Heart Center, The Christ Hospital Heart Vascular and Lung Institute, Cincinnati, Ohio, USA.
Barbra Streisand Women's Heart Center, Cedars-Sinai Smidt Heart Institute, Los Angeles, California, USA.
Womens Health Rep (New Rochelle). 2021 Apr 20;2(1):97-105. doi: 10.1089/whr.2020.0127. eCollection 2021.
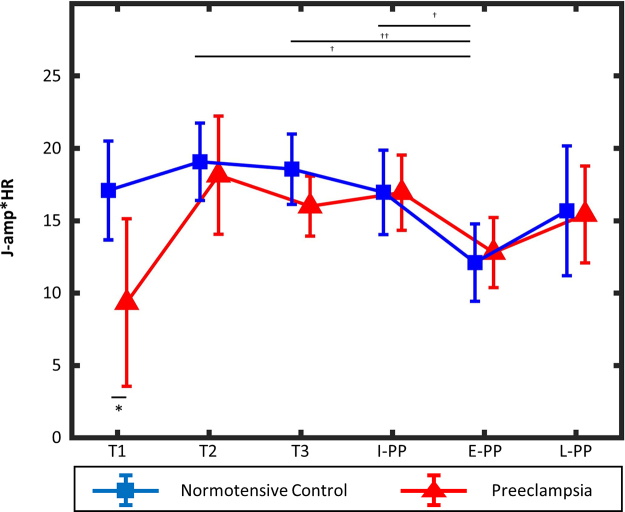
Pregnancy requires a complex physiological adaptation of the maternal cardiovascular system, which is disrupted in women with pregnancies complicated by preeclampsia, putting them at higher risk of future cardiovascular events. The measurement of body movements in response to cardiac ejection ballistocardiogram (BCG) can be used to assess cardiovascular hemodynamics noninvasively in women with preeclampsia. Using a previously validated, modified weighing scale for assessment of cardiovascular hemodynamics through measurement of BCG and electrocardiogram (ECG) signals, we collected serial measurements throughout pregnancy and postpartum and analyzed data in 30 women with preeclampsia and 23 normotensive controls. Using BCG and ECG signals, we extracted measures of cardiac output, J-wave amplitude × heart rate (J-amp × HR). Mixed-effect models with repeated measures were used to compare J-amp × HRs between groups at different time points in pregnancy and postpartum. In normotensive controls, the J-amp × HR was significantly lower early postpartum (E-PP) compared with the second trimester (T2; = 0.016) and third trimester (T3; = 0.001). Women with preeclampsia had a significantly lower J-amp × HR compared with normotensive controls during the first trimester (T1; = 0.026). In the preeclampsia group, there was a trend toward an increase in J-amp × HR from T1 to T2 and then a drop in J-amp × HR at T3 and further drop at E-PP. We observe cardiac hemodynamic changes consistent with those reported using well-validated tools. In pregnancies complicated by preeclampsia, the maximal force of contraction is lower, suggesting lower cardiac output and a trend in hemodynamics consistent with the hyperdynamic disease model of preeclampsia.
怀孕需要母体心血管系统进行复杂的生理适应,而患有子痫前期并发症的孕妇的这种适应过程会受到干扰,使她们未来发生心血管事件的风险更高。通过测量心脏射血后身体运动的弹道心动图(BCG)可用于无创评估子痫前期女性的心血管血流动力学。我们使用先前验证过的改良体重秤,通过测量BCG和心电图(ECG)信号来评估心血管血流动力学,在整个孕期和产后收集了连续测量数据,并对30名单纯收缩期高血压女性和23名血压正常的对照者的数据进行了分析。利用BCG和ECG信号,我们提取了心输出量、J波振幅×心率(J-amp×HR)的测量值。采用重复测量的混合效应模型来比较孕期和产后不同时间点两组之间的J-amp×HR。在血压正常的对照者中,产后早期(E-PP)的J-amp×HR显著低于孕中期(T2;P=0.016)和孕晚期(T3;P=0.001)。与血压正常的对照者相比,子痫前期女性在孕早期(T1)的J-amp×HR显著更低(P=0.026)。在子痫前期组中,J-amp×HR从T1到T2有增加趋势,然后在T3下降,在E-PP进一步下降。我们观察到的心脏血流动力学变化与使用经过充分验证的工具所报告的变化一致。在患有子痫前期并发症的妊娠中,最大收缩力较低,提示心输出量较低,且血流动力学趋势与子痫前期的高动力疾病模型一致。