Division of Cardiology, Department of Medicine, University of Washington, Seattle.
American Heart Association, Dallas, Texas.
JAMA Netw Open. 2021 May 3;4(5):e218828. doi: 10.1001/jamanetworkopen.2021.8828.
In-hospital mortality rates from COVID-19 are high but appear to be decreasing for selected locations in the United States. It is not known whether this is because of changes in the characteristics of patients being admitted.
To describe changing in-hospital mortality rates over time after accounting for individual patient characteristics.
DESIGN, SETTING, AND PARTICIPANTS: This was a retrospective cohort study of 20 736 adults with a diagnosis of COVID-19 who were included in the US American Heart Association COVID-19 Cardiovascular Disease Registry and admitted to 107 acute care hospitals in 31 states from March through November 2020. A multiple mixed-effects logistic regression was then used to estimate the odds of in-hospital death adjusted for patient age, sex, body mass index, and medical history as well as vital signs, use of supplemental oxygen, presence of pulmonary infiltrates at admission, and hospital site.
In-hospital death adjusted for exposures for 4 periods in 2020.
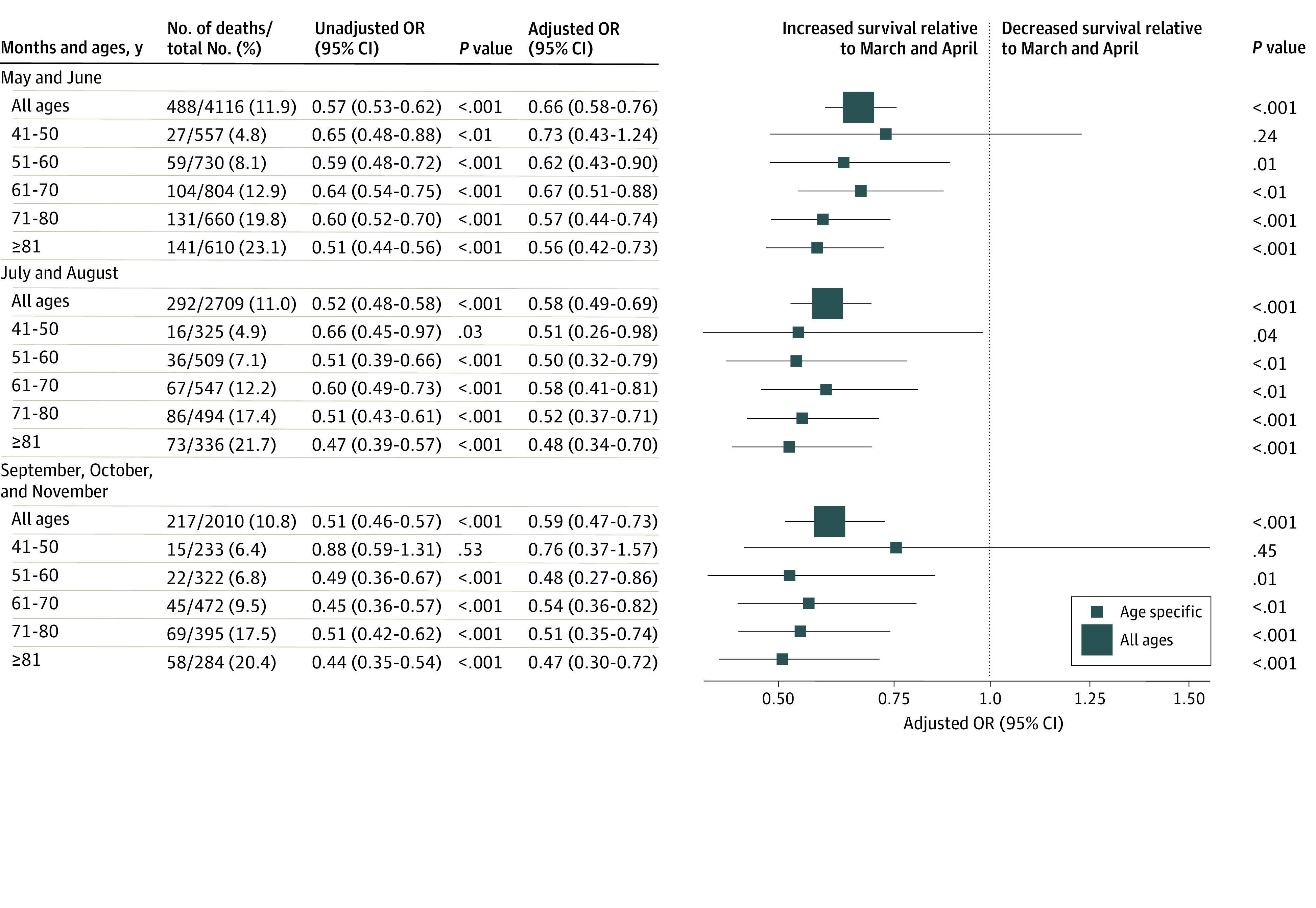
The registry included 20 736 patients hospitalized with COVID-19 from March through November 2020 (9524 women [45.9%]; mean [SD] age, 61.2 [17.9] years); 3271 patients (15.8%) died in the hospital. Mortality rates were 19.1% in March and April, 11.9% in May and June, 11.0% in July and August, and 10.8% in September through November. Compared with March and April, the adjusted odds ratios for in-hospital death were significantly lower in May and June (odds ratio, 0.66; 95% CI, 0.58-0.76; P < .001), July and August (odds ratio, 0.58; 95% CI, 0.49-0.69; P < .001), and September through November (odds ratio, 0.59; 95% CI, 0.47-0.73).
In this cohort study, high rates of in-hospital COVID-19 mortality among registry patients in March and April 2020 decreased by more than one-third by June and remained near that rate through November. This difference in mortality rates between the months of March and April and later months persisted even after adjusting for age, sex, medical history, and COVID-19 disease severity and did not appear to be associated with changes in the characteristics of patients being admitted.
美国部分地区的 COVID-19 住院死亡率较高,但似乎呈下降趋势。尚不清楚这是否是因为入院患者特征发生了变化。
描述在考虑个体患者特征后,随时间推移 COVID-19 住院死亡率的变化。
设计、地点和参与者:这是一项回顾性队列研究,纳入了美国心脏协会 COVID-19 心血管疾病登记处中的 20736 名成人 COVID-19 患者,他们于 2020 年 3 月至 11 月期间被收入美国 31 个州的 107 家急性护理医院,这些患者均被诊断为 COVID-19。然后使用多项混合效应逻辑回归来估计校正了患者年龄、性别、体重指数和既往病史以及生命体征、补充氧气使用、入院时肺部浸润存在情况和医院位置等因素后的住院死亡率。
校正了 2020 年 4 个时期的暴露因素的住院死亡率。
该登记处纳入了 2020 年 3 月至 11 月期间因 COVID-19 住院的 20736 名患者(9524 名女性[45.9%];平均[标准差]年龄为 61.2[17.9]岁);3271 名(15.8%)患者在医院死亡。3 月和 4 月的死亡率为 19.1%,5 月和 6 月为 11.9%,7 月和 8 月为 11.0%,9 月至 11 月为 10.8%。与 3 月和 4 月相比,5 月和 6 月(比值比,0.66;95%置信区间,0.58-0.76;P < .001)、7 月和 8 月(比值比,0.58;95%置信区间,0.49-0.69;P < .001)以及 9 月至 11 月(比值比,0.59;95%置信区间,0.47-0.73)住院死亡率的校正比值比显著降低。
在这项队列研究中,2020 年 3 月和 4 月登记处患者 COVID-19 住院死亡率较高,到 6 月已下降三分之一以上,此后一直保持在接近该水平,直至 11 月。3 月和 4 月与之后月份之间死亡率的这种差异在调整了年龄、性别、既往病史和 COVID-19 疾病严重程度等因素后仍然存在,且似乎与入院患者特征的变化无关。