Watad Abdulla, De Marco Gabriele, Mahajna Hussein, Druyan Amit, Eltity Mailam, Hijazi Nizar, Haddad Amir, Elias Muna, Zisman Devy, Naffaa Mohammad E, Brodavka Michal, Cohen Yael, Abu-Much Arsalan, Abu Elhija Muhanad, Bridgewood Charlie, Langevitz Pnina, McLorinan Joanna, Bragazzi Nicola Luigi, Marzo-Ortega Helena, Lidar Merav, Calabrese Cassandra, Calabrese Leonard, Vital Edward, Shoenfeld Yehuda, Amital Howard, McGonagle Dennis
Department of Medicine 'B, Zabludowicz Center for Autoimmune Diseases, Sheba Medical Center, Tel-Hashomer 10457, Israel.
Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv 69978, Israel.
Vaccines (Basel). 2021 Apr 29;9(5):435. doi: 10.3390/vaccines9050435.
Infectious diseases and vaccines can occasionally cause new-onset or flare of immune-mediated diseases (IMDs). The adjuvanticity of the available SARS-CoV-2 vaccines is based on either TLR-7/8 or TLR-9 agonism, which is distinct from previous vaccines and is a common pathogenic mechanism in IMDs.
We evaluated IMD flares or new disease onset within 28-days of SARS-CoV-2 vaccination at five large tertiary centres in countries with early vaccination adoption, three in Israel, one in UK, and one in USA. We assessed the pattern of disease expression in terms of autoimmune, autoinflammatory, or mixed disease phenotype and organ system affected. We also evaluated outcomes.
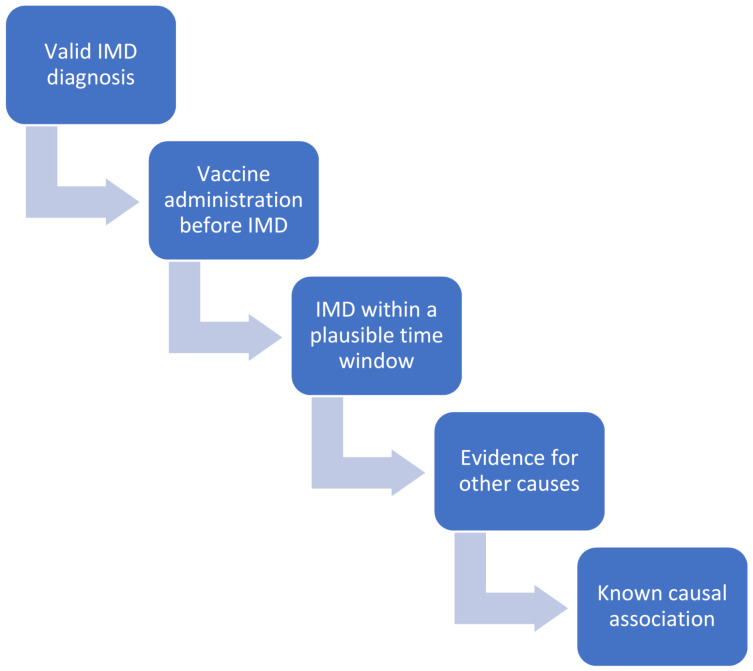
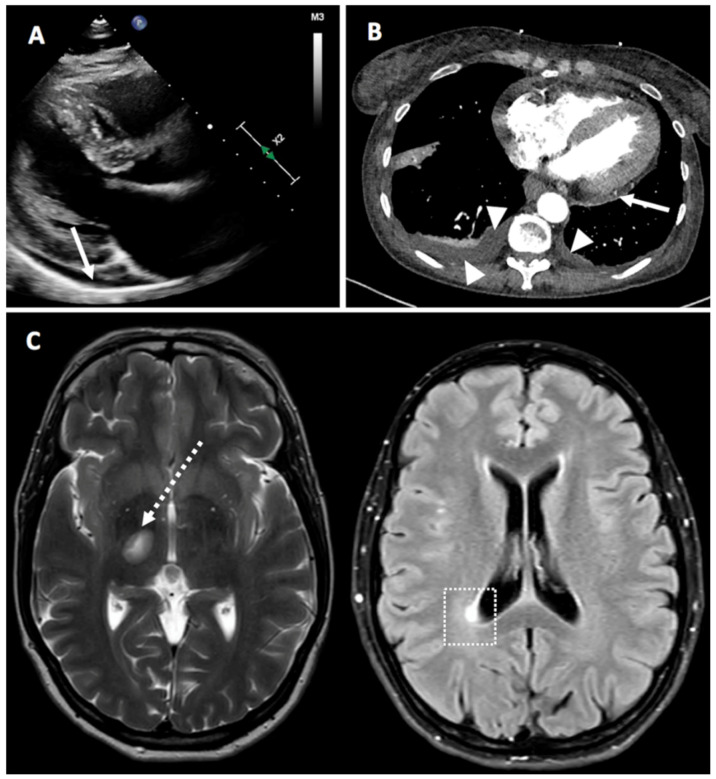
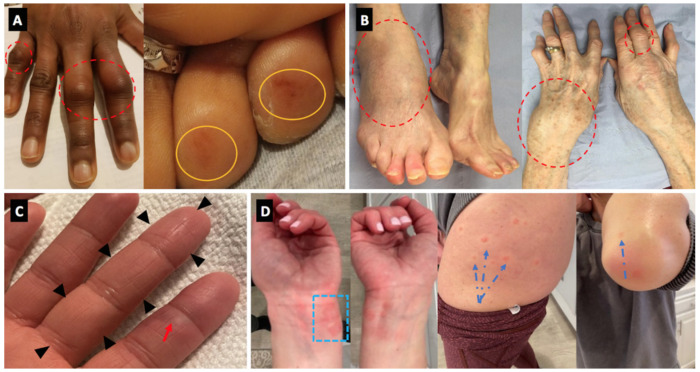
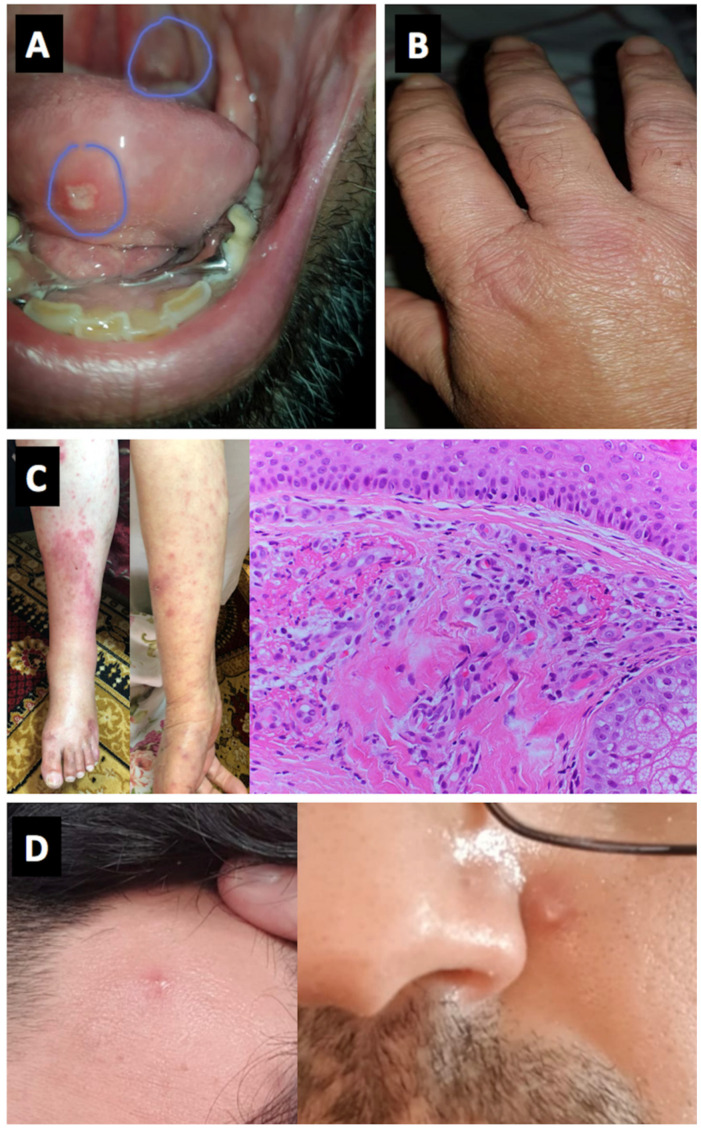
27 cases included 17 flares and 10 new onset IMDs. 23/27 received the BNT - 162b2 vaccine, 2/27 the mRNA-1273 and 2/27 the ChAdOx1 vaccines. The mean age was 54.4 ± 19.2 years and 55% of cases were female. Among the 27 cases, 21 (78%) had at least one underlying autoimmune/rheumatic disease prior the vaccination. Among those patients with a flare or activation, four episodes occurred after receiving the second-dose and in one patient they occurred both after the first and the second-dose. In those patients with a new onset disease, two occurred after the second-dose and in one patient occurred both after the first (new onset) and second-dose (flare). For either dose, IMDs occurred on average 4 days later. Of the cases, 20/27 (75%) were mild to moderate in severity. Over 80% of cases had excellent resolution of inflammatory features, mostly with the use of corticosteroid therapy. Other immune-mediated conditions included idiopathic pericarditis ( = 2), neurosarcoidosis with small fiber neuropathy ( = 1), demyelination ( = 1), and myasthenia gravis ( = 2). In 22 cases (81.5%), the insurgence of Adverse event following immunization (AEFI)/IMD could not be explained based on the drug received by the patient. In 23 cases (85.2%), AEFI development could not be explained based on the underlying disease/co-morbidities. Only in one case (3.7%), the timing window of the insurgence of the side effect was considered not compatible with the time from vaccine to flare.
Despite the high population exposure in the regions served by these centers, IMDs flares or onset temporally-associated with SARS-CoV-2 vaccination appear rare. Most are moderate in severity and responsive to therapy although some severe flares occurred.
none.
传染病和疫苗偶尔会引发免疫介导疾病(IMD)的新发或病情加重。现有的严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗的佐剂活性基于Toll样受体7/8(TLR-7/8)或TLR-9激动作用,这与先前的疫苗不同,是免疫介导疾病的一种常见致病机制。
我们在五个早期采用疫苗接种的国家的大型三级中心评估了SARS-CoV-2疫苗接种后28天内IMD病情加重或新发疾病的情况,其中三个在以色列,一个在英国,一个在美国。我们根据自身免疫性、自身炎症性或混合性疾病表型以及受影响的器官系统评估了疾病表现模式。我们还评估了结果。
27例病例包括17例病情加重和10例新发IMD。27例中有23例接种了BNT-162b2疫苗,2例接种了mRNA-1273疫苗,2例接种了ChAdOx1疫苗。平均年龄为54.4±19.2岁,55%的病例为女性。在这27例病例中,21例(78%)在接种疫苗前至少有一种潜在的自身免疫性/风湿性疾病。在那些病情加重或激活的患者中,4例在接种第二剂后出现,1例在接种第一剂和第二剂后均出现。在那些新发疾病的患者中,2例在接种第二剂后出现,1例在接种第一剂(新发)和第二剂后(病情加重)均出现。对于任一剂次,IMD平均在4天后发生。在这些病例中,20/27(75%)的严重程度为轻度至中度。超过80%的病例炎症特征得到了很好的缓解,大多采用了皮质类固醇治疗。其他免疫介导的疾病包括特发性心包炎(=2)、伴有小纤维神经病变的神经结节病(=1)、脱髓鞘(=1)和重症肌无力(=2)。在22例(81.5%)病例中,免疫接种后不良事件(AEFI)/IMD的发生无法根据患者所接种的药物来解释。在23例(85.2%)病例中,AEFI的发生无法根据潜在疾病/合并症来解释。仅在1例(3.7%)病例中,副作用发生的时间窗被认为与从疫苗接种到病情加重的时间不相符。
尽管这些中心所服务地区的人群暴露率很高,但与SARS-CoV-2疫苗接种在时间上相关的IMD病情加重或发病似乎很少见。大多数严重程度为中度,对治疗有反应,尽管也发生了一些严重的病情加重情况。
无。