Heart Failure, Mechanical Circulatory Support and Transplant (P.S., M.P., M.A.S., F.L., N.I., W.Z., C.W.M.), Inova Heart and Vascular Institute, Falls Church, Virginia.
Utah Transplant Affiliated Hospitals (U.T.A.H.) Cardiac Transplant Program, University of Utah Health and School of Medicine, Intermountain Medical Center and Salt Lake Veterans Affairs Medical Center (I.T., R.A., O.W.-P., M.Y., J.S., J.C.F., C.P.K., L.B.C., S.S.D., C.H.S., A.K., S.G.D.).
Circ Heart Fail. 2021 May;14(5):e007991. doi: 10.1161/CIRCHEARTFAILURE.120.007991. Epub 2021 May 5.
Variable definitions and an incomplete understanding of the gradient of reverse cardiac remodeling following continuous flow left ventricular assist device (LVAD) implantation has limited the field of myocardial plasticity. We evaluated the continuum of LV remodeling by serial echocardiographic imaging to define 3 stages of reverse cardiac remodeling following LVAD.
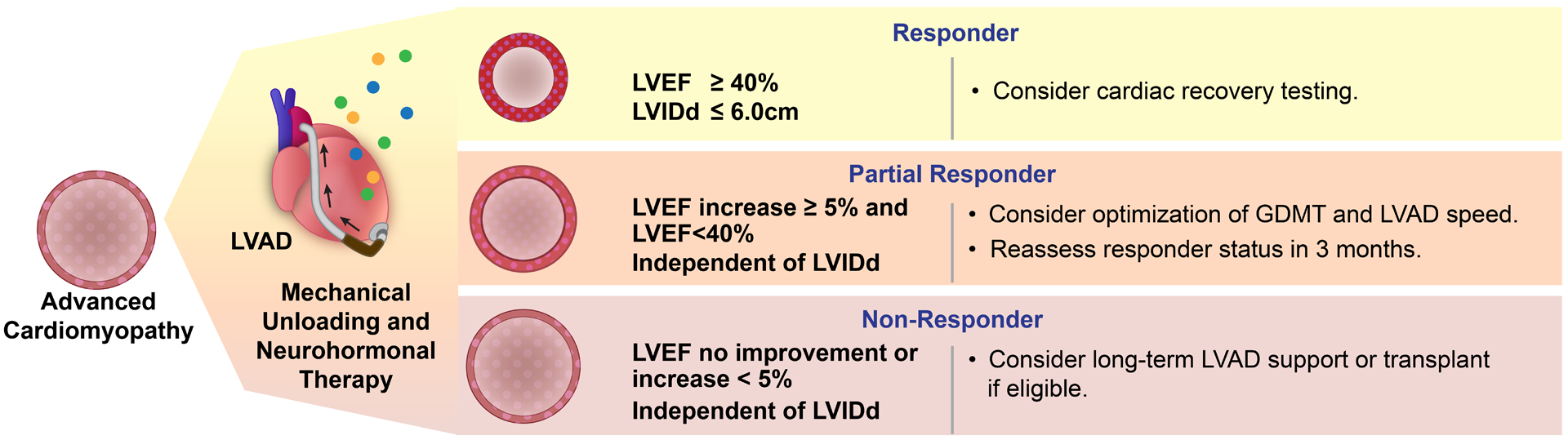
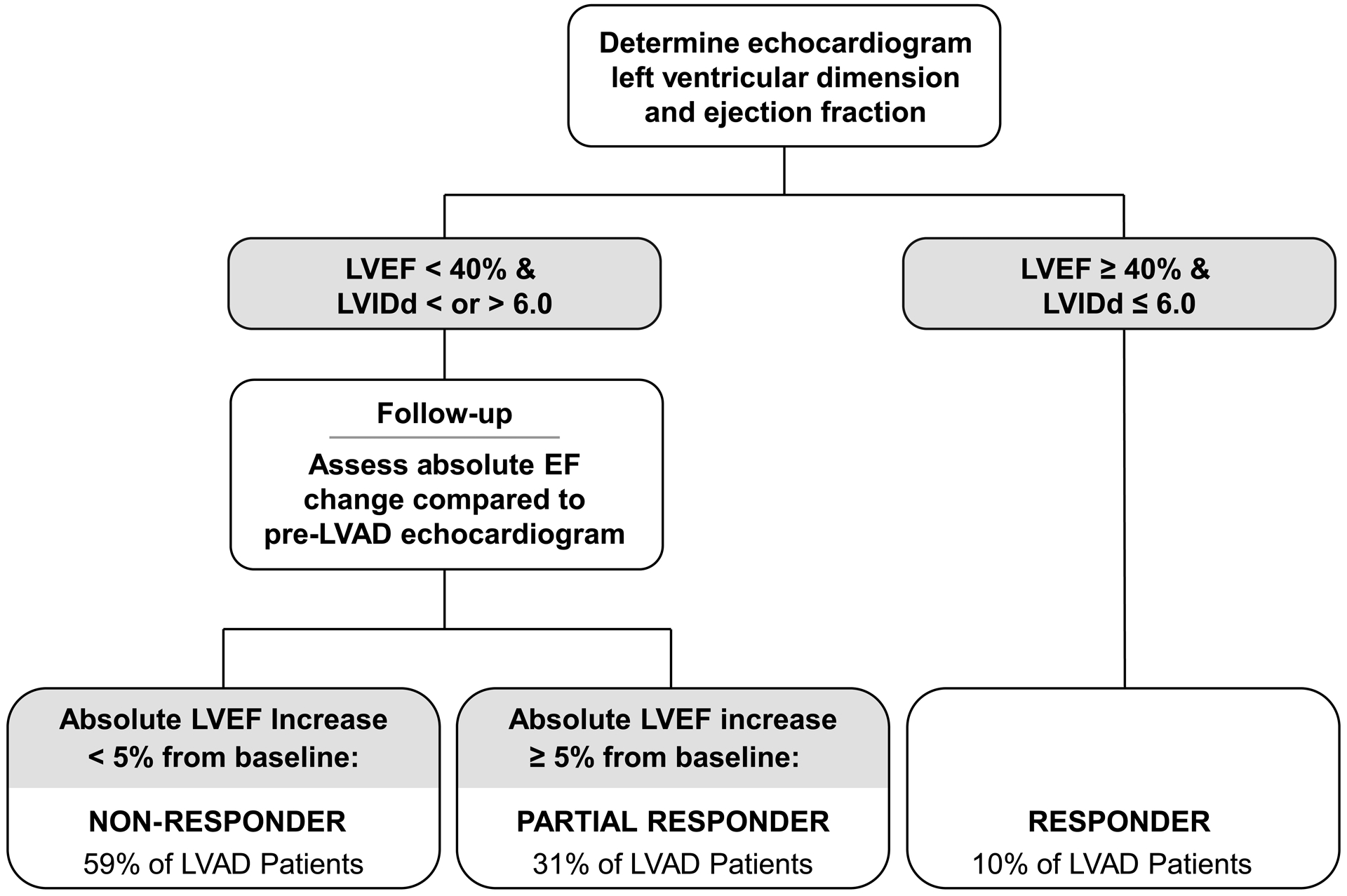
The study enrolled consecutive LVAD patients across 4 study sites. A blinded echocardiographer evaluated the degree of structural (LV internal dimension at end-diastole [LVIDd]) and functional (LV ejection fraction [LVEF]) change after LVAD. Patients experiencing an improvement in LVEF ≥40% and LVIDd ≤6.0 cm were termed responders, absolute change in LVEF of ≥5% and LVEF <40% were termed partial responders, and the remaining patients with no significant improvement in LVEF were termed nonresponders.
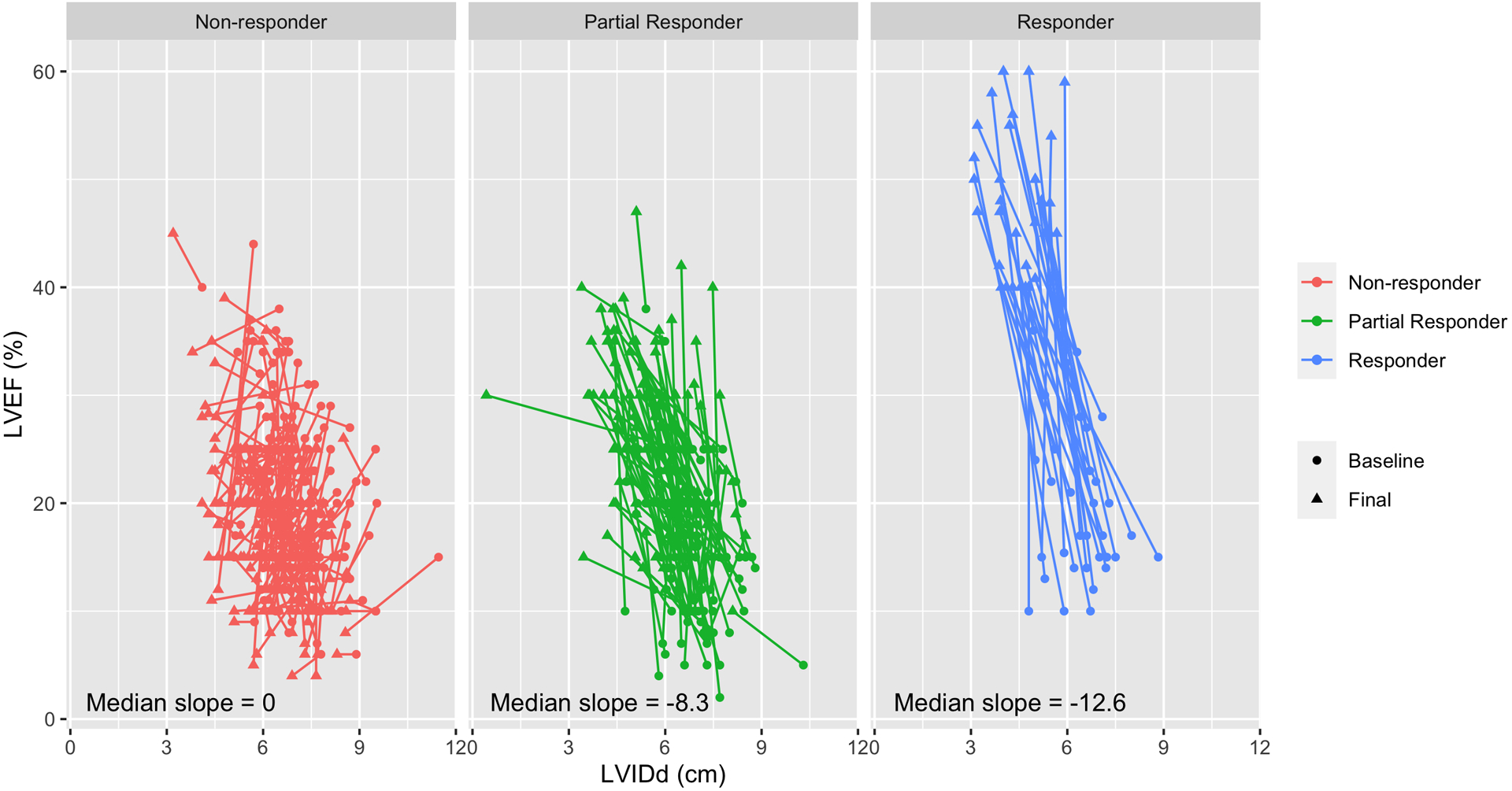
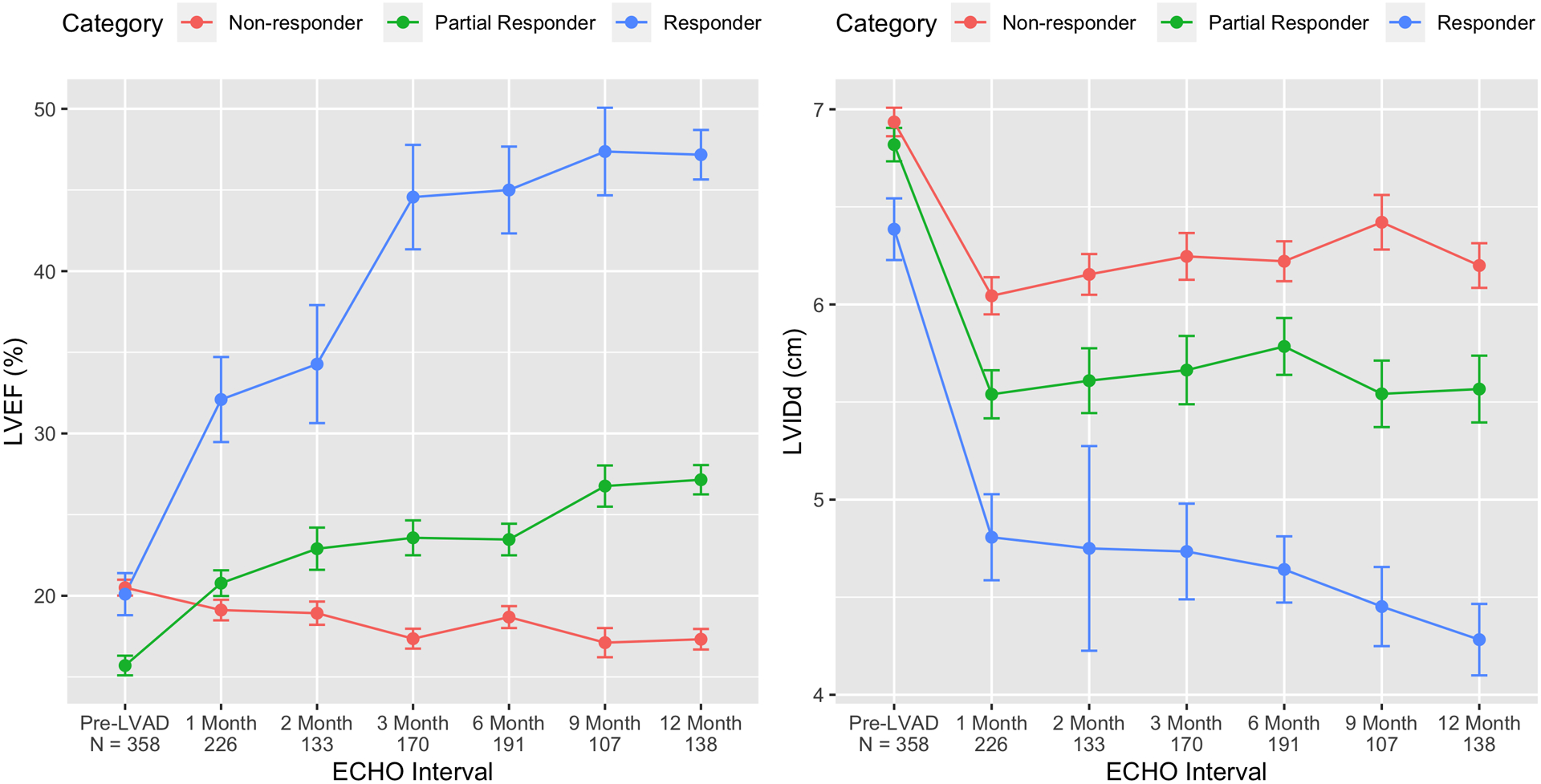
Among 358 LVAD patients, 34 (10%) were responders, 112 (31%) partial responders, and the remaining 212 (59%) were nonresponders. The use of guideline-directed medical therapy for heart failure was higher in partial responders and responders. Structural changes (LVIDd) followed a different pattern with significant improvements even in patients who had minimal LVEF improvement. With mechanical unloading, the median reduction in LVIDd was -0.6 cm (interquartile range [IQR], -1.1 to -0.1 cm; nonresponders), -1.1 cm (IQR, -1.8 to -0.4 cm; partial responders), and -1.9 cm (IQR, -2.9 to -1.1 cm; responders). Similarly, the median change in LVEF was -2% (IQR, -6% to 1%), 9% (IQR, 6%-14%), and 27% (IQR, 23%-33%), respectively.
Reverse cardiac remodeling associated with durable LVAD support is not an all-or-none phenomenon and manifests in a continuous spectrum. Defining 3 stages across this continuum can inform clinical management, facilitate the field of myocardial plasticity, and improve the design of future investigations.
由于变量定义不明确以及对连续流动左心室辅助装置(LVAD)植入后逆向心脏重构梯度的理解不完整,限制了心肌可塑性领域的发展。我们通过连续超声心动图成像评估 LV 重构的连续体,以定义 LVAD 后逆向心脏重构的 3 个阶段。
该研究在 4 个研究地点连续招募了 LVAD 患者。一位经过盲法培训的超声心动图医师评估了 LVAD 后结构(LV 舒张末期内径 [LVIDd])和功能(LV 射血分数 [LVEF])变化的程度。LVAD 后 LVEF 改善≥40%且 LVIDd≤6.0 cm 的患者被称为反应者,LVEF 绝对变化≥5%且 LVEF<40%的患者被称为部分反应者,而其余 LVEF 无明显改善的患者被称为无反应者。
在 358 例 LVAD 患者中,34 例(10%)为反应者,112 例(31%)为部分反应者,其余 212 例(59%)为无反应者。部分反应者和反应者使用指南指导的心力衰竭药物治疗的比例更高。结构变化(LVIDd)呈现出不同的模式,即使在 LVEF 改善最小的患者中也有明显改善。随着机械卸载,LVIDd 的中位数减少量分别为-0.6 cm(四分位距 [IQR],-1.1 至-0.1 cm;无反应者)、-1.1 cm(IQR,-1.8 至-0.4 cm;部分反应者)和-1.9 cm(IQR,-2.9 至-1.1 cm;反应者)。同样,LVEF 的中位数变化分别为-2%(IQR,-6%至 1%)、9%(IQR,6%-14%)和 27%(IQR,23%-33%)。
与持久的 LVAD 支持相关的逆向心脏重构不是一种全有或全无的现象,而是表现为一个连续的谱。在这个连续体上定义 3 个阶段可以为临床管理提供信息,促进心肌可塑性领域的发展,并改进未来研究的设计。