Campbell-Sills Laura, Sun Xiaoying, Choi Karmel W, He Feng, Ursano Robert J, Kessler Ronald C, Levey Daniel F, Smoller Jordan W, Gelernter Joel, Jain Sonia, Stein Murray B
Department of Psychiatry, University of California San Diego, La Jolla, CA, USA.
Biostatistics Research Center, Herbert Wertheim School of Public Health and Human Longevity Science, University of California San Diego, La Jolla, CA, USA.
Psychol Med. 2021 May 5;52(15):1-9. doi: 10.1017/S0033291721000428.
Definition of disorder subtypes may facilitate precision treatment for posttraumatic stress disorder (PTSD). We aimed to identify PTSD subtypes and evaluate their associations with genetic risk factors, types of stress exposures, comorbidity, and course of PTSD.
Data came from a prospective study of three U.S. Army Brigade Combat Teams that deployed to Afghanistan in 2012. Soldiers with probable PTSD (PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition ≥31) at three months postdeployment comprised the sample (N = 423) for latent profile analysis using Gaussian mixture modeling and PTSD symptom ratings as indicators. PTSD profiles were compared on polygenic risk scores (derived from external genomewide association study summary statistics), experiences during deployment, comorbidity at three months postdeployment, and persistence of PTSD at nine months postdeployment.
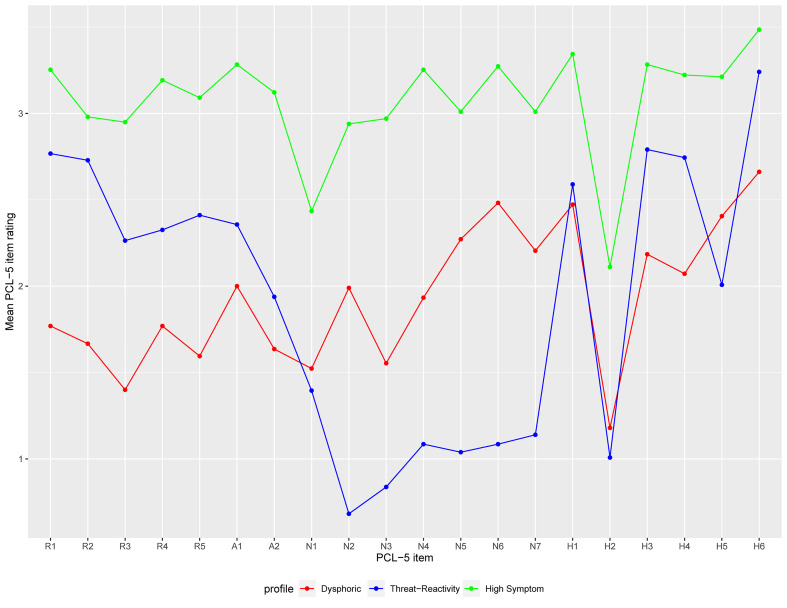
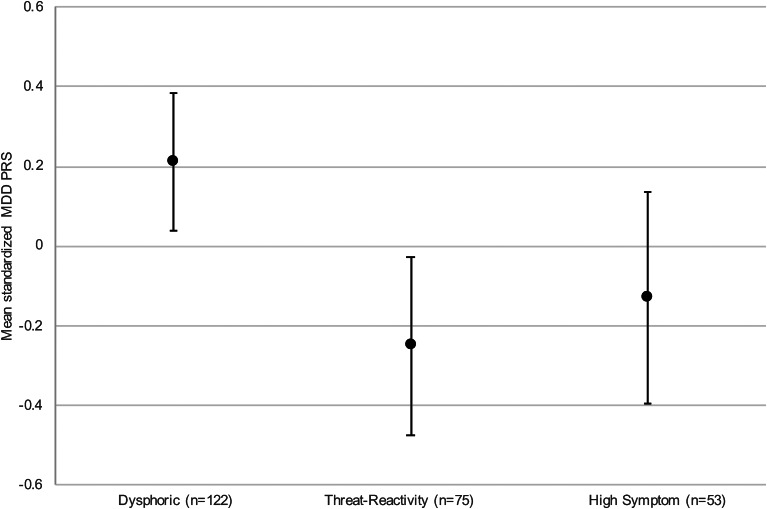
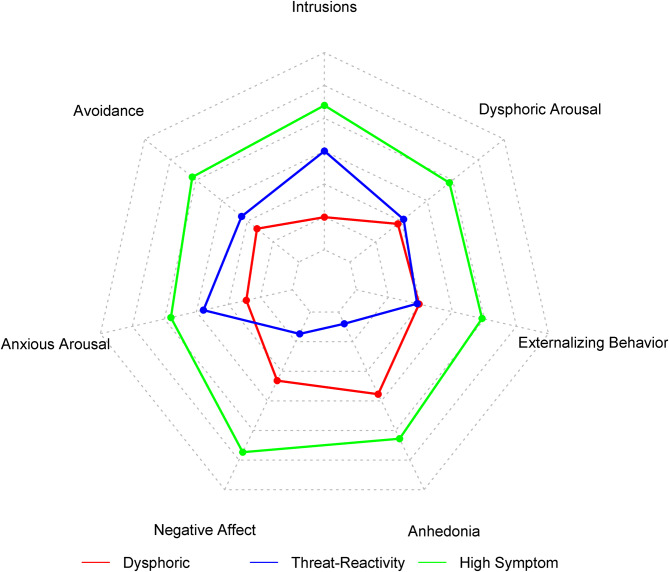
Latent profile analysis revealed profiles characterized by prominent intrusions, avoidance, and hyperarousal (threat-reactivity profile; n = 129), anhedonia and negative affect (dysphoric profile; n = 195), and high levels of all PTSD symptoms (high-symptom profile; n = 99). The threat-reactivity profile had the most combat exposure and the least comorbidity. The dysphoric profile had the highest polygenic risk for major depression, and more personal life stress and co-occurring major depression than the threat-reactivity profile. The high-symptom profile had the highest rates of concurrent mental disorders and persistence of PTSD.
Genetic and trauma-related factors likely contribute to PTSD heterogeneity, which can be parsed into subtypes that differ in symptom expression, comorbidity, and course. Future studies should evaluate whether PTSD typology modifies treatment response and should clarify distinctions between the dysphoric profile and depressive disorders.
创伤后应激障碍(PTSD)亚型的定义可能有助于精准治疗。我们旨在识别PTSD亚型,并评估它们与遗传风险因素、应激暴露类型、共病情况及PTSD病程的关联。
数据来自于对2012年部署到阿富汗的三个美国陆军旅战斗队的一项前瞻性研究。部署后三个月时可能患有PTSD(《精神疾病诊断与统计手册(第五版)》PTSD检查表≥31)的士兵构成了样本(N = 423),使用高斯混合模型和PTSD症状评分作为指标进行潜在类别分析。比较了PTSD类别在多基因风险评分(源自外部全基因组关联研究汇总统计数据)、部署期间的经历、部署后三个月的共病情况以及部署后九个月时PTSD持续存在情况方面的差异。
潜在类别分析揭示了以突出闯入、回避和过度警觉为特征(威胁反应型;n = 129)、快感缺失和消极情绪为特征(烦躁型;n = 195)以及所有PTSD症状水平都高为特征(高症状型;n = 99)这几种类别。威胁反应型战斗暴露最多,共病最少。烦躁型患重度抑郁症的多基因风险最高,与威胁反应型相比,有更多的个人生活应激和共病的重度抑郁症。高症状型并发精神障碍和PTSD持续存在的发生率最高。
遗传因素和与创伤相关因素可能导致PTSD的异质性,这可以解析为在症状表现、共病情况和病程方面存在差异的亚型。未来的研究应评估PTSD类型学是否会改变治疗反应,并应阐明烦躁型与抑郁症之间的区别。