Department of Laboratory Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of Immunology, School of Basic Medicine, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Front Immunol. 2021 Apr 19;12:641378. doi: 10.3389/fimmu.2021.641378. eCollection 2021.
Inadequate tuberculosis (TB) diagnostics, especially for discrimination between active TB (ATB) and latent TB infection (LTBI), are major hurdle in the reduction of the disease burden. The present study aims to investigate the role of lymphocyte non-specific function detection for TB diagnosis in clinical practice.
A total of 208 participants including 49 ATB patients, 64 LTBI individuals, and 95 healthy controls were recruited at Tongji hospital from January 2019 to October 2020. All subjects were tested with lymphocyte non-specific function detection and T-SPOT assay.
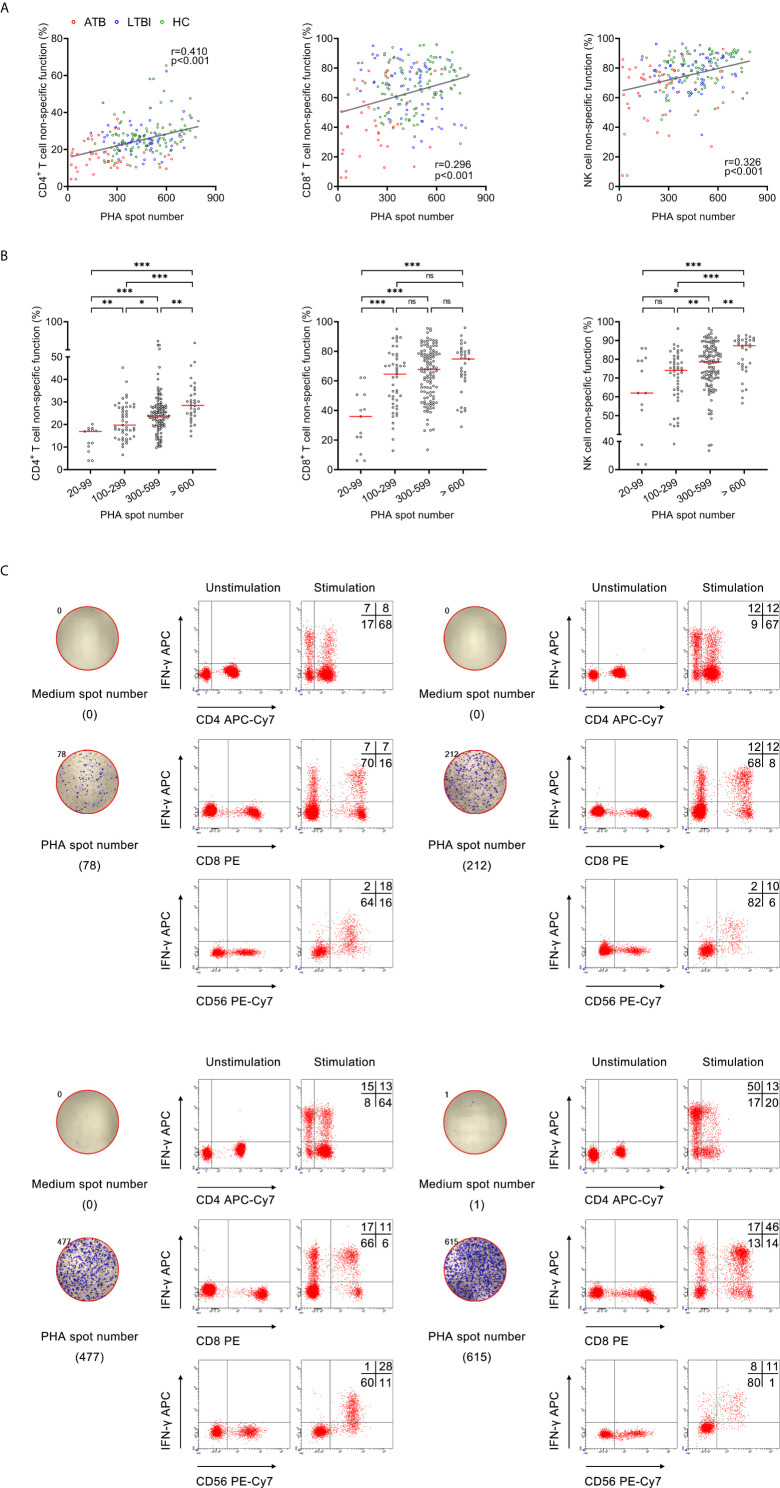
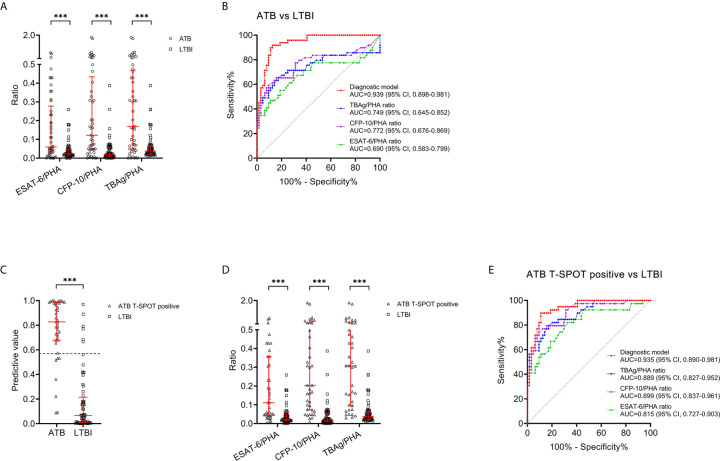
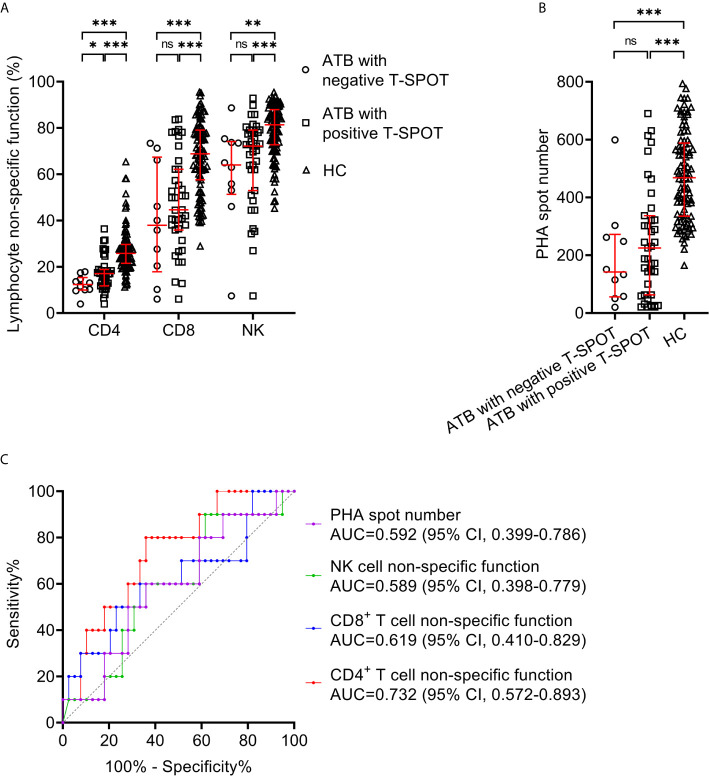
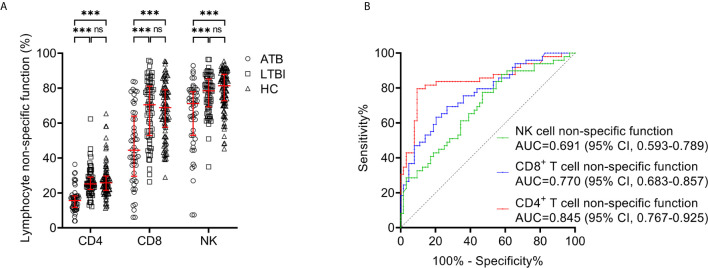
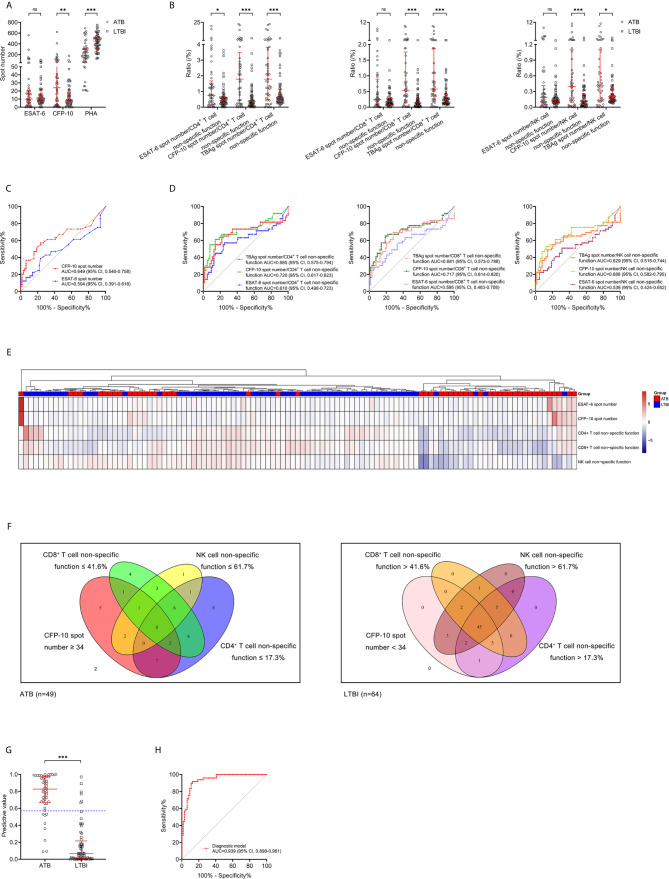
Significantly positive correlation existed between lymphocyte non-specific function and phytohemagglutinin (PHA) spot number. CD4 T cell non-specific function showed the potential for differentiating patients with negative T-SPOT results from those with positive T-SPOT results with an area under the curve (AUC) of 0.732 (95% CI, 0.572-0.893). The non-specific function of CD4 T cells, CD8 T cells, and NK cells was found significantly lower in ATB patients than in LTBI individuals. The AUCs presented by CD4 T cell non-specific function, CD8 T cell non-specific function, and NK cell non-specific function for discriminating ATB patients from LTBI individuals were 0.845 (95% CI, 0.767-0.925), 0.770 (95% CI, 0.683-0.857), and 0.691 (95% CI, 0.593-0.789), respectively. Application of multivariable logistic regression resulted in the combination of CD4 T cell non-specific function, NK cell non-specific function, and culture filtrate protein-10 (CFP-10) spot number as the optimally diagnostic model for differentiating ATB from LTBI. The AUC of the model in distinguishing between ATB and LTBI was 0.939 (95% CI, 0.898-0.981). The sensitivity and specificity were 83.67% (95% CI, 70.96%-91.49%) and 90.63% (95% CI, 81.02%-95.63%) with the threshold as 0.57. Our established model showed superior performance to TB-specific antigen (TBAg)/PHA ratio in stratifying TB infection status.
Lymphocyte non-specific function detection offers an attractive alternative to facilitate TB diagnosis. The three-index diagnostic model was proved to be a potent tool for the identification of different events involved in TB infection, which is helpful for the treatment and management of patients.
结核病(TB)诊断不足,尤其是区分活动性 TB(ATB)和潜伏性 TB 感染(LTBI),是降低疾病负担的主要障碍。本研究旨在探讨淋巴细胞非特异性功能检测在临床实践中对 TB 诊断的作用。
2019 年 1 月至 2020 年 10 月,共招募了 208 名参与者,包括 49 名 ATB 患者、64 名 LTBI 个体和 95 名健康对照者。所有受试者均接受淋巴细胞非特异性功能检测和 T-SPOT 检测。
淋巴细胞非特异性功能与植物血凝素(PHA)斑点数呈显著正相关。CD4 T 细胞非特异性功能显示出区分 T-SPOT 结果阴性和阳性患者的潜力,曲线下面积(AUC)为 0.732(95%置信区间,0.572-0.893)。与 LTBI 个体相比,ATB 患者的 CD4 T 细胞、CD8 T 细胞和 NK 细胞的非特异性功能明显降低。CD4 T 细胞非特异性功能、CD8 T 细胞非特异性功能和 NK 细胞非特异性功能区分 ATB 患者和 LTBI 个体的 AUC 分别为 0.845(95%置信区间,0.767-0.925)、0.770(95%置信区间,0.683-0.857)和 0.691(95%置信区间,0.593-0.789)。多变量逻辑回归的应用得出结论,CD4 T 细胞非特异性功能、NK 细胞非特异性功能和培养滤液蛋白-10(CFP-10)斑点数的组合是区分 ATB 和 LTBI 的最佳诊断模型。该模型在区分 ATB 和 LTBI 方面的 AUC 为 0.939(95%置信区间,0.898-0.981)。其阈值为 0.57,灵敏度和特异性分别为 83.67%(95%置信区间,70.96%-91.49%)和 90.63%(95%置信区间,81.02%-95.63%)。与 TB 特异性抗原(TBAg)/PHA 比值相比,我们建立的模型在分层 TB 感染状态方面表现出更好的性能。
淋巴细胞非特异性功能检测为 TB 诊断提供了一种有吸引力的替代方法。三指标诊断模型被证明是一种区分 TB 感染不同事件的有效工具,有助于患者的治疗和管理。