Department of Infectious Disease and and Institute of Global Health and Innovation, Division of Medicine, Imperial College, London, UK.
Kilifi County Hospital and Kenya Medical Research Institute (KEMRI) Wellcome Trust Research Programme, Kilifi, Kenya.
Intensive Care Med. 2021 May;47(5):566-576. doi: 10.1007/s00134-021-06385-3. Epub 2021 May 5.
The life-saving role of oxygen therapy in African children with severe pneumonia is not yet established.
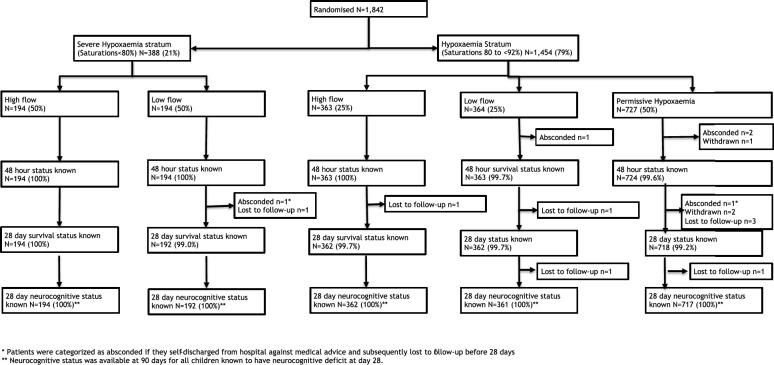
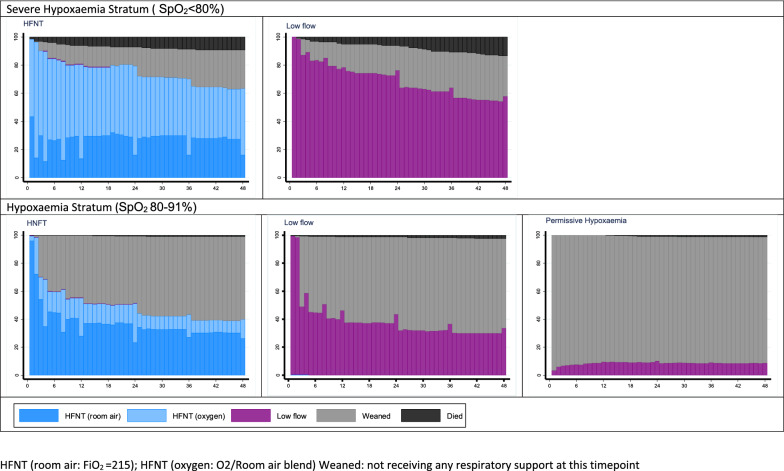
The open-label fractional-factorial COAST trial randomised eligible Ugandan and Kenyan children aged > 28 days with severe pneumonia and severe hypoxaemia stratum (SpO < 80%) to high-flow nasal therapy (HFNT) or low-flow oxygen (LFO: standard care) and hypoxaemia stratum (SpO 80-91%) to HFNT or LFO (liberal strategies) or permissive hypoxaemia (ratio 1:1:2). Children with cyanotic heart disease, chronic lung disease or > 3 h receipt of oxygen were excluded. The primary endpoint was 48 h mortality; secondary endpoints included mortality or neurocognitive sequelae at 28 days.
The trial was stopped early after enrolling 1852/4200 children, including 388 in the severe hypoxaemia stratum (median 7 months; median SpO 75%) randomised to HFNT (n = 194) or LFO (n = 194) and 1454 in the hypoxaemia stratum (median 9 months; median SpO 88%) randomised to HFNT (n = 363) vs LFO (n = 364) vs permissive hypoxaemia (n = 727). Per-protocol 15% of patients in the permissive hypoxaemia group received oxygen (when SpO < 80%). In the severe hypoxaemia stratum, 48-h mortality was 9.3% for HFNT vs. 13.4% for LFO groups. In the hypoxaemia stratum, 48-h mortality was 1.1% for HFNT vs. 2.5% LFO and 1.4% for permissive hypoxaemia. In the hypoxaemia stratum, adjusted odds ratio for 48-h mortality in liberal vs permissive comparison was 1.16 (0.49-2.74; p = 0.73); HFNT vs LFO comparison was 0.60 (0.33-1.06; p = 0.08). Strata-specific 28 day mortality rates were, respectively: 18.6, 23.4 and 3.3, 4.1, 3.9%. Neurocognitive sequelae were rare.
Respiratory support with HFNT showing potential benefit should prompt further trials.
在患有严重肺炎的非洲儿童中,氧疗的救生作用尚未得到证实。
这项开放标签的分层因子 COAST 试验将符合条件的乌干达和肯尼亚患有严重肺炎和严重低氧血症(SpO < 80%)的 28 天以上的儿童随机分为高流量鼻治疗(HFNT)或低流量氧气(LFO:标准护理)组和低氧血症组(SpO 80-91%)HFNT 或 LFO(自由策略)或允许性低氧血症(比例 1:1:2)组。患有紫绀型先天性心脏病、慢性肺部疾病或接受氧气治疗超过 3 小时的儿童被排除在外。主要终点是 48 小时死亡率;次要终点包括 28 天的死亡率或神经认知后遗症。
在招募了 4200 名儿童中的 1852 名儿童后,该试验提前停止,其中 388 名严重低氧血症患儿(中位数 7 个月;中位数 SpO 75%)被随机分为 HFNT(n = 194)或 LFO(n = 194)组,1454 名低氧血症患儿(中位数 9 个月;中位数 SpO 88%)被随机分为 HFNT(n = 363)与 LFO(n = 364)组和允许性低氧血症组(n = 727)。在允许性低氧血症组中,15%的患者按方案接受了氧气治疗(当 SpO < 80%)。在严重低氧血症组中,HFNT 组的 48 小时死亡率为 9.3%,LFO 组为 13.4%。在低氧血症组中,HFNT 组的 48 小时死亡率为 1.1%,LFO 组为 2.5%,允许性低氧血症组为 1.4%。在低氧血症组中,48 小时死亡率的调整比值比为自由与允许性比较为 1.16(0.49-2.74;p = 0.73);HFNT 与 LFO 比较为 0.60(0.33-1.06;p = 0.08)。特定于层的 28 天死亡率分别为:18.6、23.4 和 3.3、4.1、3.9%。神经认知后遗症很少见。
HFNT 显示出潜在益处的呼吸支持应促使进一步的试验。