Division of Infectious Disease, Department of Medicine, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States of America.
William S. Middleton Memorial Veterans Hospital, Madison, WI, United States of America.
PLoS One. 2021 May 6;16(5):e0251170. doi: 10.1371/journal.pone.0251170. eCollection 2021.
The recovery of other pathogens in patients with SARS-CoV-2 infection has been reported, either at the time of a SARS-CoV-2 infection diagnosis (co-infection) or subsequently (superinfection). However, data on the prevalence, microbiology, and outcomes of co-infection and superinfection are limited. The purpose of this study was to examine the occurrence of co-infections and superinfections and their outcomes among patients with SARS-CoV-2 infection.
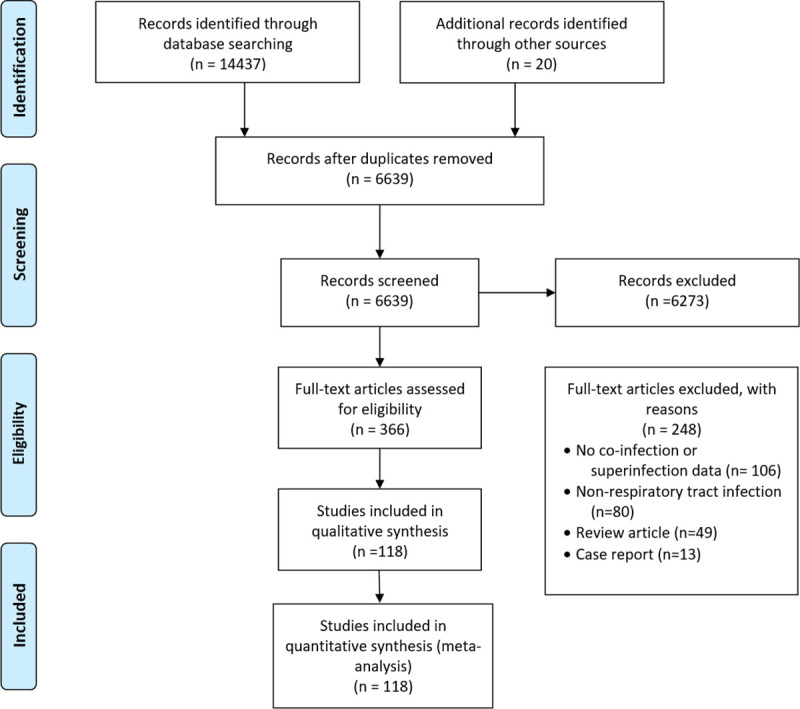
We searched literature databases for studies published from October 1, 2019, through February 8, 2021. We included studies that reported clinical features and outcomes of co-infection or superinfection of SARS-CoV-2 and other pathogens in hospitalized and non-hospitalized patients. We followed PRISMA guidelines, and we registered the protocol with PROSPERO as: CRD42020189763.
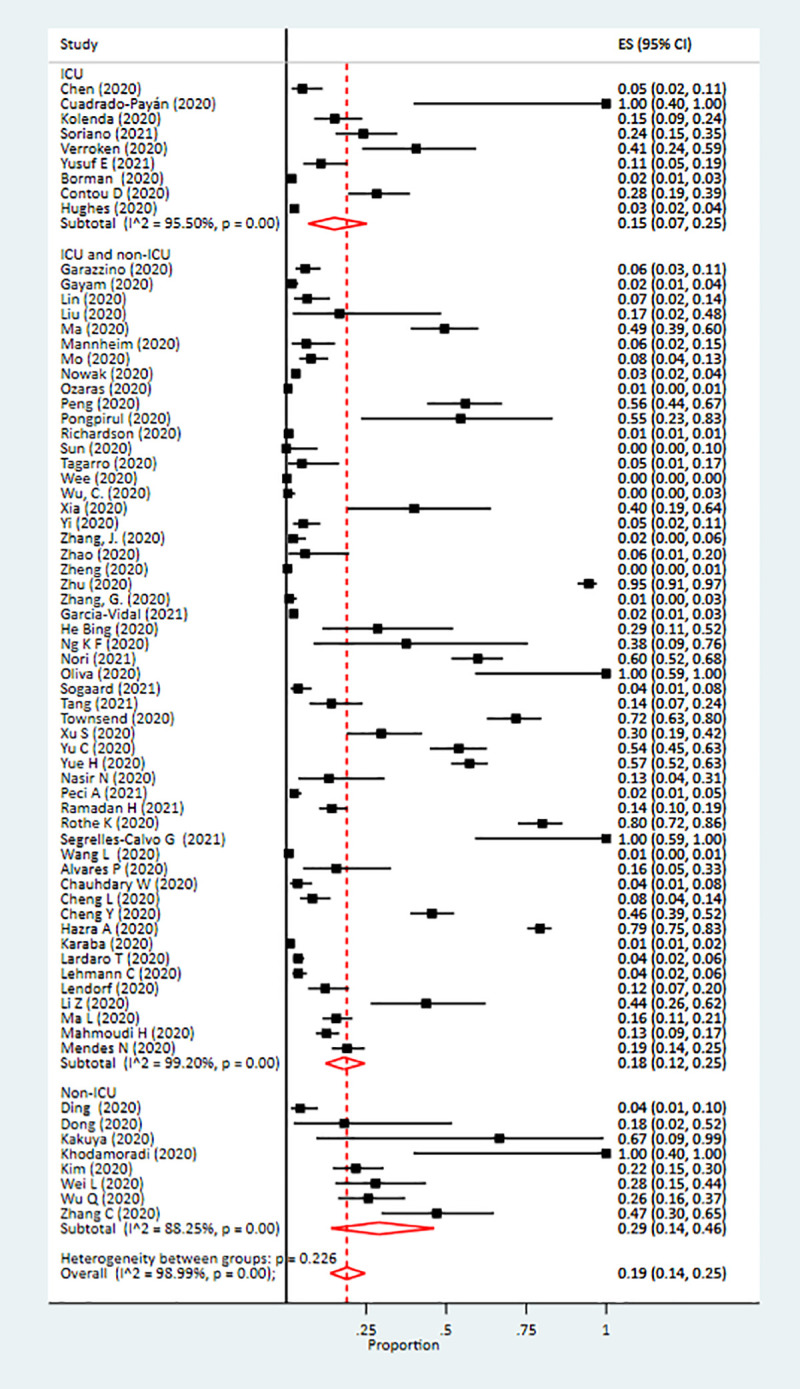
Of 6639 articles screened, 118 were included in the random effects meta-analysis. The pooled prevalence of co-infection was 19% (95% confidence interval [CI]: 14%-25%, I2 = 98%) and that of superinfection was 24% (95% CI: 19%-30%). Pooled prevalence of pathogen type stratified by co- or superinfection were: viral co-infections, 10% (95% CI: 6%-14%); viral superinfections, 4% (95% CI: 0%-10%); bacterial co-infections, 8% (95% CI: 5%-11%); bacterial superinfections, 20% (95% CI: 13%-28%); fungal co-infections, 4% (95% CI: 2%-7%); and fungal superinfections, 8% (95% CI: 4%-13%). Patients with a co-infection or superinfection had higher odds of dying than those who only had SARS-CoV-2 infection (odds ratio = 3.31, 95% CI: 1.82-5.99). Compared to those with co-infections, patients with superinfections had a higher prevalence of mechanical ventilation (45% [95% CI: 33%-58%] vs. 10% [95% CI: 5%-16%]), but patients with co-infections had a greater average length of hospital stay than those with superinfections (mean = 29.0 days, standard deviation [SD] = 6.7 vs. mean = 16 days, SD = 6.2, respectively).
Our study showed that as many as 19% of patients with COVID-19 have co-infections and 24% have superinfections. The presence of either co-infection or superinfection was associated with poor outcomes, including increased mortality. Our findings support the need for diagnostic testing to identify and treat co-occurring respiratory infections among patients with SARS-CoV-2 infection.
已报道在 SARS-CoV-2 感染患者中存在其他病原体的恢复,无论是在 SARS-CoV-2 感染诊断时(合并感染)还是随后(继发感染)。然而,关于合并感染和继发感染的流行率、微生物学和结局的数据有限。本研究旨在检查 SARS-CoV-2 感染患者中合并感染和继发感染的发生情况及其结局。
我们检索了 2019 年 10 月 1 日至 2021 年 2 月 8 日期间发表的文献数据库。我们纳入了报告 SARS-CoV-2 与其他病原体合并感染或继发感染的临床特征和结局的住院和非住院患者的研究。我们遵循 PRISMA 指南,并在 PROSPERO 中注册了方案:CRD42020189763。
在筛选出的 6639 篇文章中,有 118 篇被纳入随机效应荟萃分析。合并感染的患病率为 19%(95%置信区间[CI]:14%-25%,I2 = 98%),继发感染的患病率为 24%(95% CI:19%-30%)。按合并或继发感染分层的病原体类型的合并患病率为:病毒合并感染 10%(95% CI:6%-14%);病毒继发感染 4%(95% CI:0%-10%);细菌合并感染 8%(95% CI:5%-11%);细菌继发感染 20%(95% CI:13%-28%);真菌合并感染 4%(95% CI:2%-7%);真菌继发感染 8%(95% CI:4%-13%)。合并感染或继发感染的患者死亡的可能性高于仅感染 SARS-CoV-2 的患者(比值比=3.31,95% CI:1.82-5.99)。与合并感染相比,继发感染患者更有可能需要机械通气(45%[95% CI:33%-58%] vs. 10%[95% CI:5%-16%]),但合并感染患者的平均住院时间长于继发感染患者(均值=29.0 天,标准差[SD]=6.7 vs. 均值=16 天,SD=6.2)。
我们的研究表明,多达 19%的 COVID-19 患者存在合并感染,24%存在继发感染。合并感染或继发感染的存在与不良结局相关,包括死亡率增加。我们的研究结果支持对 SARS-CoV-2 感染患者进行诊断性检测,以识别和治疗同时发生的呼吸道感染。