University of Toronto, Toronto, Ontario, Canada.
University Health Network, Toronto, Ontario, Canada.
PLoS One. 2021 May 6;16(5):e0251334. doi: 10.1371/journal.pone.0251334. eCollection 2021.
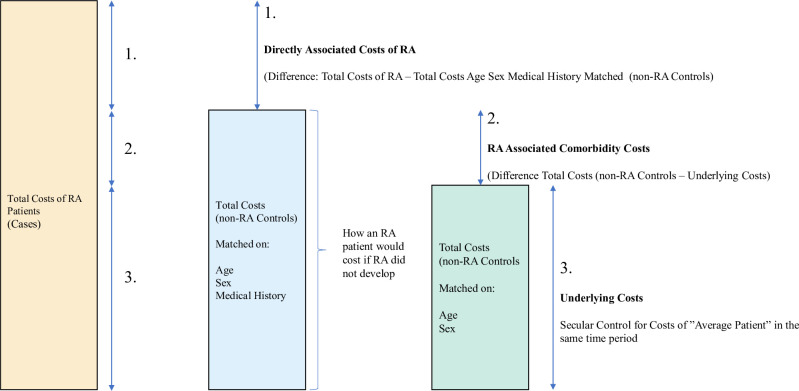
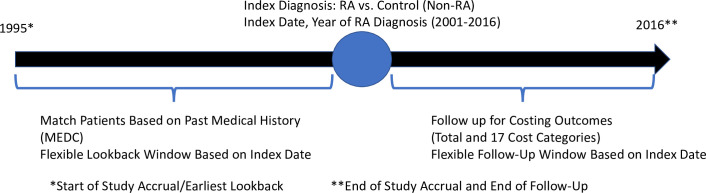
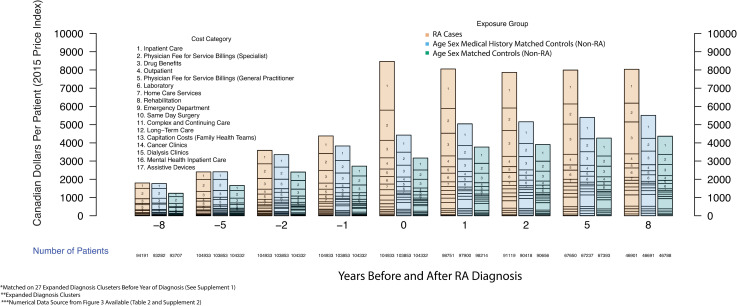
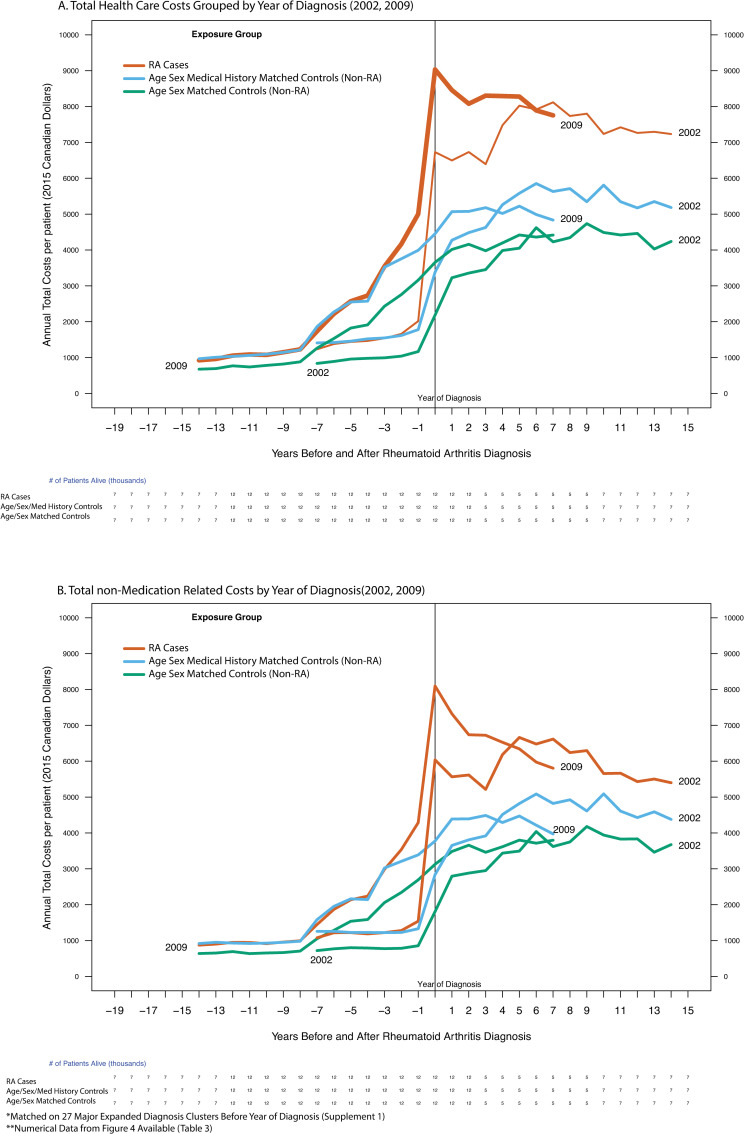
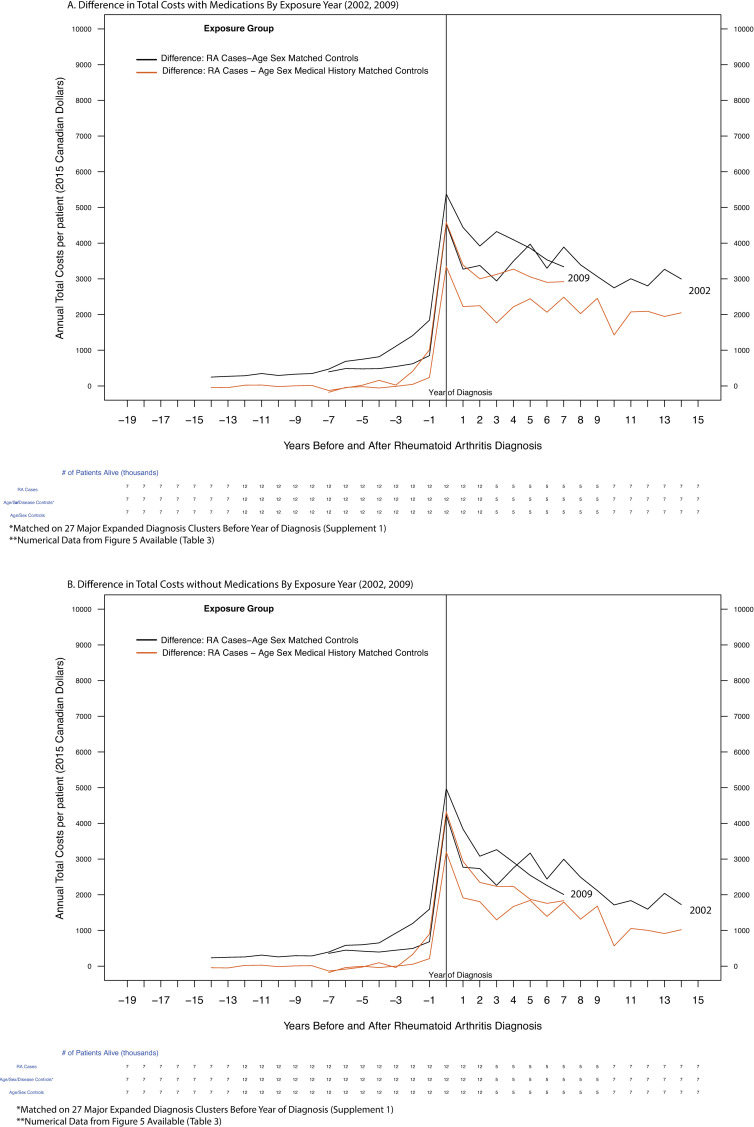
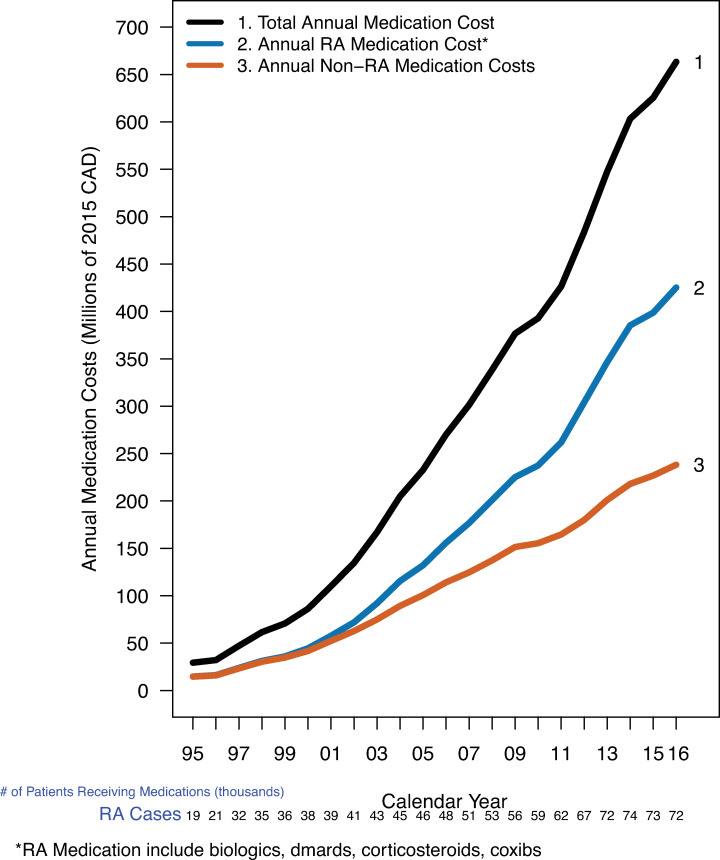
Quantifying the contribution of rheumatoid arthritis to the acquisition of subsequent health care costs is an emerging focus of the rheumatologic community and payers of health care. Our objective was to determine the healthcare costs before and after diagnosis of rheumatoid arthritis (RA) from the public payer's perspective. The study design was a longitudinal observational administrative data-based cohort with RA cases from Ontario Canada (n = 104,933) and two control groups, matched 1:1 on year of cohort entry from 2001 to 2016. The first control group was matched on age, sex and calendar year of cohort entry (diagnosis year for those with RA); the second group added medical history to the match before RA diagnosis year. The main exposure was new onset RA. The secondary exposure was calendar year of RA diagnosis to compare attributable costs over the study observation window. Main outcomes were health care costs in 2015 Canadian dollars, overall and by cost category. We used attribution methods to classify costs into those associated with RA, those associated with comorbidities, and age/sex-related underlying costs. Health care costs associated with RA increased up to the year of diagnosis, where they reached $8,591: $4,142 in RA associated costs; $1,242 in RA comorbidity associated costs; and $3,207 in underlying costs. In the eighth-year post diagnosis, the RA costs declined to $2,567 while the RA comorbidity associated costs remained relatively constant at $1,142, and the underlying age/sex related cost increased to $4,426. RA patients had lower costs when diagnosed in later calendar years. Our results suggest a large proportion of disease related health care costs are a result of costs associated with RA comorbidities, which may appear many years before diagnosis.
从公共支付方的角度定量评估类风湿关节炎(RA)对后续医疗保健费用的影响,是风湿学界和医疗保健支付方关注的新兴焦点。我们的目的是确定从公共支付方的角度看,RA 患者在确诊前和确诊后的医疗保健费用。研究设计为基于纵向观察性行政数据的队列研究,纳入了来自加拿大安大略省的 RA 病例(n=104933)和两个对照组,每个对照组均与 RA 患者按年份匹配(2001 年至 2016 年)。第一个对照组按年龄、性别和 RA 患者的入组年份(即诊断年份)进行匹配;第二个对照组在 RA 诊断年份之前增加了病史匹配。主要暴露因素为新发 RA。次要暴露因素为 RA 诊断年份,用于比较研究观察窗口内的归因成本。主要结局为 2015 年加元的医疗保健费用,包括总体费用和按费用类别分类的费用。我们使用归因方法将成本分为与 RA 相关的成本、与合并症相关的成本和与年龄/性别相关的基础成本。与 RA 相关的医疗保健费用在诊断当年达到高峰,为 8591 加元:其中 4142 加元为 RA 相关成本;1242 加元为 RA 合并症相关成本;3207 加元为与年龄/性别相关的基础成本。在诊断后第 8 年,RA 相关成本降至 2567 加元,而 RA 合并症相关成本保持相对稳定(1142 加元),与年龄/性别相关的基础成本增加至 4426 加元。RA 患者在较晚的年份确诊时,成本较低。我们的研究结果表明,很大一部分疾病相关医疗保健费用是 RA 合并症相关成本的结果,这些成本可能在诊断前多年就已出现。