Li Shijie, Lu Shiyang, Liu Xuefeng, Chen Xiaonan
Department of Urology, Shengjing Hospital of China Medical University, Shenyang, China.
Front Oncol. 2021 Apr 20;11:664392. doi: 10.3389/fonc.2021.664392. eCollection 2021.
Serum albumin-to-alkaline phosphatase ratio (AAPR) has been proven to be a prognostic indicator of many malignant tumors. However, whether it can predict the prognosis of bladder cancer (BC) patients who underwent radical cystectomy (RC) remains unclear. This study was designed to assess the relationship between AAPR and clinical outcomes in patients with BC treated with RC.
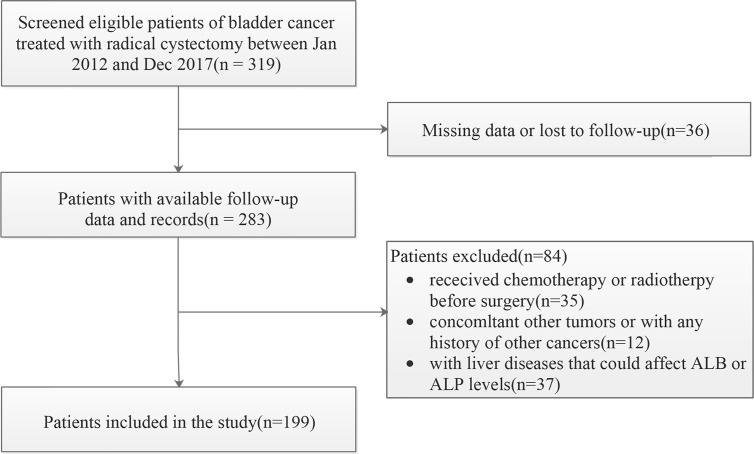
The clinicopathological data of 199 BC patients receiving RC in our institution from January 2012 to December 2017 were retrospectively collected and analyzed. They were divided into three groups based on the optimal cut-off values and the association between AAPR groups and their clinical outcomes were evaluated.
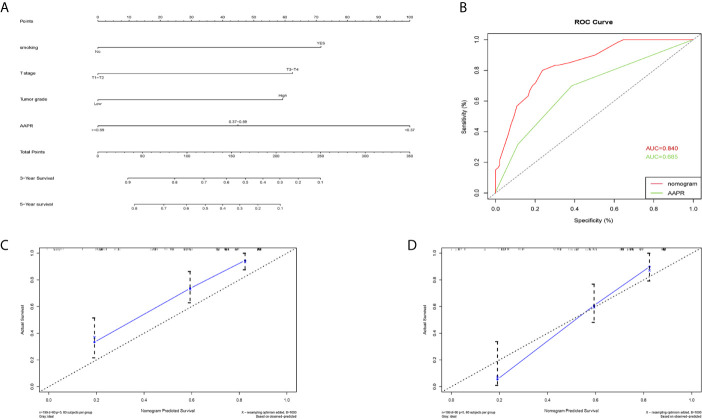
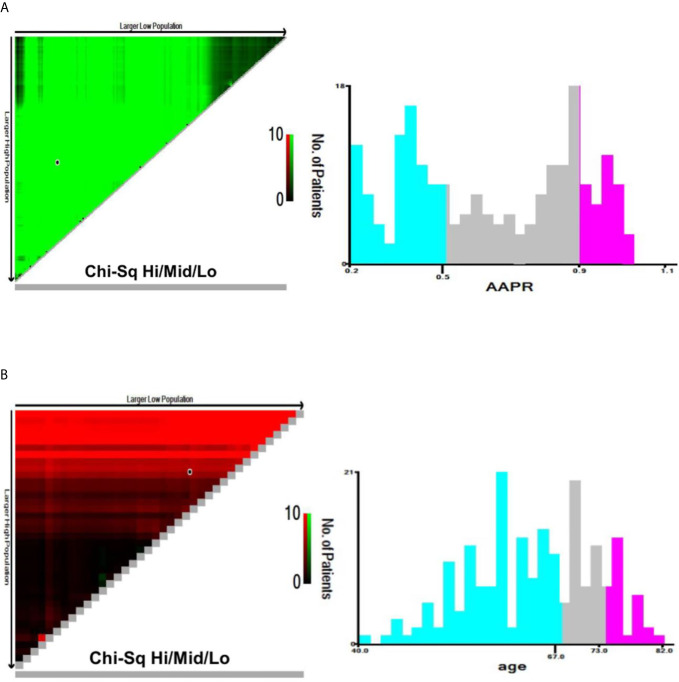
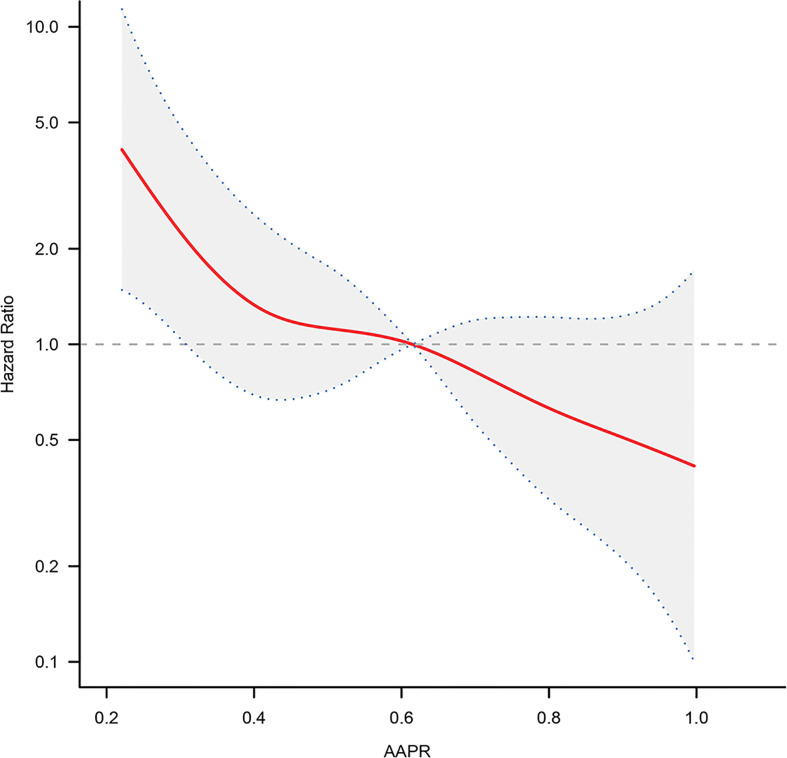
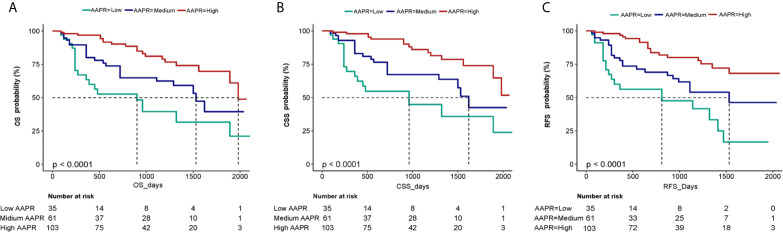
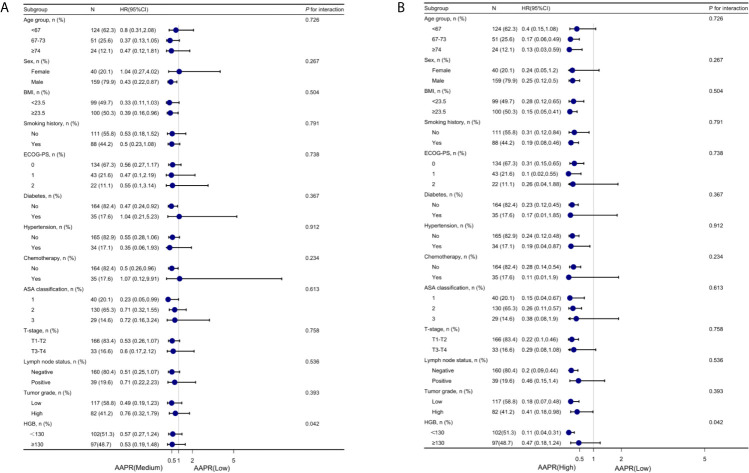
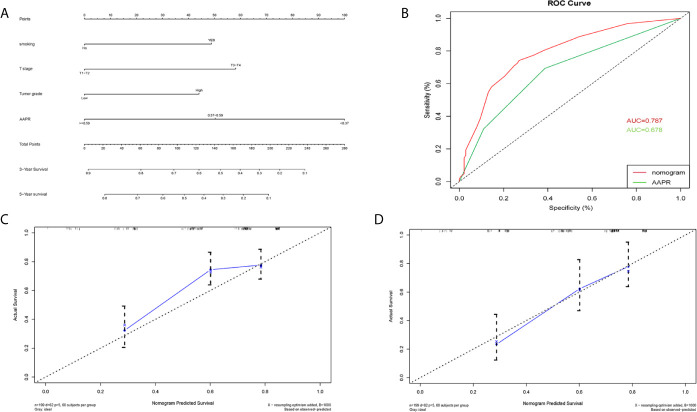
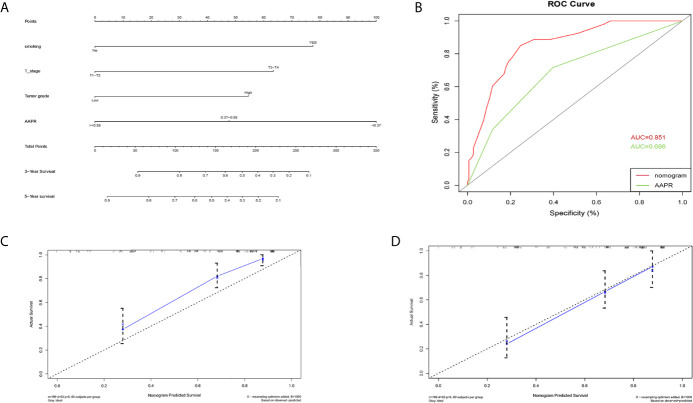
The average age of the patients was (64.0 ± 8.7) years and 79.9% were male. Based on the cut-off values of AAPR, patients were divided into three groups: low-AAPR group (AAPR < 0.37, n = 35), medium-AAPR group (AAPR = 0.37-0.59, n = 61) and high-AAPR group (AAPR > 0.59, n = 103). The median overall survival (OS) of each AAPR group was 12.5, 24, and 29 months, respectively ( value <0.0001). After adjusting the Cox proportional hazards model, medium- and high- AAPR groups showed a reduced risk trend of death, with a risk ratio of 0.44 (95% CI = 0.21-0.91) and 0.25 (95% CI = 0.12-0.49), respectively ( for trend <0.001). No nonlinear relationship was identified by smooth fitting curve between AAPR and OS. By subgroup analysis, we observed that compared to the low-AAPR group, the trends of the HRs in the medium- and high-AAPR group were decreased across nearly all subgroups after stratification. Moreover, the AAPR-based nomograms for OS, CSS and RFS were also constructed. The C-index showed a good predictive accuracy (OS, C-index 0.728, 95% CI 0.663-0.793; CSS, C-index 0.792, 95% CI 0.748-0.838; RFS, C-index 0.784, 95% CI 0.739-0.829).
Pretreatment AAPR is significantly associated with the prognosis of BC patients receiving RC, which can be conducive to the clinical decision-making and risk stratification in those patients. The nomogram based on AAPR is a reliable model for predicting survival of BC patients after RC.
血清白蛋白与碱性磷酸酶比值(AAPR)已被证明是多种恶性肿瘤的预后指标。然而,其能否预测接受根治性膀胱切除术(RC)的膀胱癌(BC)患者的预后仍不清楚。本研究旨在评估AAPR与接受RC治疗的BC患者临床结局之间的关系。
回顾性收集并分析了2012年1月至2017年12月在我院接受RC治疗的199例BC患者的临床病理资料。根据最佳截断值将他们分为三组,并评估AAPR组与其临床结局之间的关联。
患者的平均年龄为(64.0±8.7)岁,79.9%为男性。根据AAPR的截断值,患者分为三组:低AAPR组(AAPR<0.37,n=35)、中AAPR组(AAPR=0.37-0.59,n=61)和高AAPR组(AAPR>0.59,n=103)。各AAPR组的中位总生存期(OS)分别为12.5、24和29个月(P值<0.0001)。调整Cox比例风险模型后,中、高AAPR组显示出死亡风险降低的趋势,风险比分别为0.44(95%CI=0.21-0.91)和0.25(95%CI=0.12-0.49)(趋势P<0.001)。AAPR与OS之间的平滑拟合曲线未发现非线性关系。通过亚组分析,我们观察到,与低AAPR组相比,分层后中、高AAPR组在几乎所有亚组中的HRs趋势均降低。此外,还构建了基于AAPR的OS、CSS和RFS列线图。C指数显示出良好的预测准确性(OS,C指数0.728,95%CI 0.663-0.793;CSS,C指数0.792,95%CI 0.748-0.838;RFS,C指数0.784,95%CI 0.739-0.829)。
术前AAPR与接受RC治疗的BC患者的预后显著相关,这有助于这些患者的临床决策和风险分层。基于AAPR的列线图是预测BC患者RC术后生存的可靠模型。