Department of Psychiatry and Behavioral Sciences, Stanford University, Stanford, California.
Department of Neurosurgery, Stanford University, Stanford, California.
JAMA Netw Open. 2021 May 3;4(5):e218049. doi: 10.1001/jamanetworkopen.2021.8049.
In the US and the United Kingdom, cocaine use is the second leading cause of illicit drug overdose death. Psychosocial treatments for cocaine use disorder are limited, and no pharmacotherapy is approved for use in the US or Europe.
To compare treatments for active cocaine use among adults.
PubMed and the Cochrane Database of Systematic Reviews were searched for clinical trials published between December 31, 1995, and December 31, 2017.
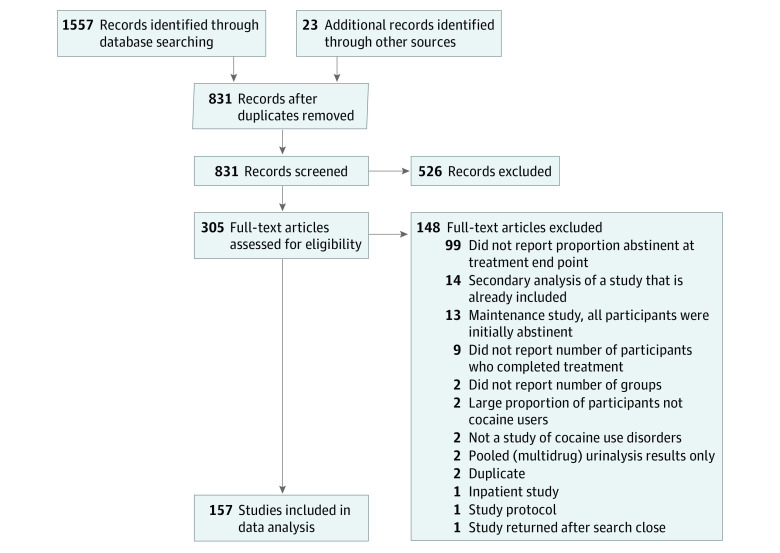
This meta-analysis was registered on Covidence.org (study 8731) on December 31, 2015. Clinical trials were included if they (1) had the term cocaine in the article title; (2) were published between December 31, 1995, and December 31, 2017; (3) were written in English; (4) enrolled outpatients 18 years or older with active cocaine use at baseline; and (5) reported treatment group size, treatment duration, retention rates, and urinalysis results for the presence of cocaine metabolites. A study was excluded if (1) more than 25% of participants were not active cocaine users or more than 80% of participants had negative test results for the presence of cocaine metabolites at baseline and (2) it reported only pooled urinalysis results indicating the presence of multiple substances and did not report the specific proportion of positive test results for cocaine metabolites. Multiple reviewers reached criteria consensus. Of 831 records screened, 157 studies (18.9%) met selection criteria and were included in the analysis.
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guideline. Search results were imported from PubMed XML into Covidence.org then Microsoft Excel. Data extraction was completed in 2 iterations to ensure fidelity. Analyses included a multilevel random-effects model, a multilevel mixed-effects meta-regression model, and sensitivity analyses. Treatments were clustered into 11 categories (psychotherapy, contingency management programs, placebo, opioids, psychostimulants, anticonvulsants, dopamine agonists, antidepressants, antipsychotics, miscellaneous medications, and other therapies). Missing data were imputed using multiple imputation by chained equations. The significance threshold for all analyses was P = .05. Data were analyzed using the metafor and mice packages in R software, version 3.3.2 (R Foundation for Statistical Computing). Data were analyzed from January 1, 2018, to February 28, 2021.
The primary outcome was the intention-to-treat logarithm of the odds ratio (OR) of having a negative urinalysis result for the presence of cocaine metabolites at the end of each treatment period compared with baseline. The hypothesis, which was formulated after data collection, was that no treatment category would have a significant association with objective reductions in cocaine use.
A total of 157 studies comprising 402 treatment groups and 15 842 participants were included. Excluding other therapies, the largest treatment groups across all studies were psychotherapy (mean [SD] number of participants, 40.04 [36.88]) and contingency management programs (mean [SD] number of participants, 37.51 [25.51]). Only contingency management programs were significantly associated with an increased likelihood of having a negative test result for the presence of cocaine (OR, 2.13; 95% CI, 1.62-2.80), and this association remained significant in all sensitivity analyses.
In this meta-analysis, contingency management programs were associated with reductions in cocaine use among adults. Research efforts and policies that align with this treatment modality may benefit those who actively use cocaine and attenuate societal burdens.
在美国和英国,可卡因的使用是导致非法药物过量死亡的第二大主要原因。针对可卡因使用障碍的心理社会治疗方法有限,并且没有药物疗法获得美国或欧洲的批准。
比较成人可卡因使用的治疗方法。
在 1995 年 12 月 31 日至 2017 年 12 月 31 日期间,在 PubMed 和 Cochrane 系统评价数据库中搜索发表的临床试验。
这项荟萃分析于 2015 年 12 月 31 日在 Covidence.org(研究 8731)上进行注册。如果临床试验符合以下标准,则将其纳入:(1)文章标题中包含“可卡因”一词;(2)发表于 1995 年 12 月 31 日至 2017 年 12 月 31 日之间;(3)用英文书写;(4)招募门诊患者,基线时为可卡因使用者;(5)报告治疗组的大小、治疗持续时间、保留率以及尿液分析结果以检测可卡因代谢物的存在。如果(1)超过 25%的参与者不是可卡因使用者,或者超过 80%的参与者在基线时可卡因代谢物的检测结果为阴性,则研究被排除在外;(2)仅报告汇总的尿液分析结果表明存在多种物质,而未报告可卡因代谢物阳性检测结果的具体比例,则研究被排除在外。多名审查员达成了标准共识。在筛选出的 831 份记录中,有 157 项研究(18.9%)符合入选标准并纳入分析。
本研究遵循系统评价和荟萃分析的首选报告项目(PRISMA)指南。从 PubMed XML 中导入搜索结果到 Covidence.org 然后到 Microsoft Excel。分两次完成数据提取以确保结果准确。分析包括多水平随机效应模型、多水平混合效应荟萃回归模型和敏感性分析。治疗方法分为 11 类(心理治疗、行为契约管理方案、安慰剂、阿片类药物、苯丙胺类兴奋剂、抗惊厥药、多巴胺激动剂、抗抑郁药、抗精神病药、其他药物和其他治疗方法)。使用 chained equations 多重插补法对缺失数据进行插补。所有分析的显著性阈值为 P =.05。使用 R 软件版本 3.3.2(R 基金会用于统计计算)中的 metafor 和 mice 包进行数据分析。数据分析从 2018 年 1 月 1 日至 2021 年 2 月 28 日进行。
主要结果是每个治疗期结束时与基线相比,尿液中可卡因代谢物检测结果为阴性的意向治疗对数比值(OR)。在数据收集后提出的假设是,没有任何治疗类别与可卡因使用的客观减少有显著关联。
共有 157 项研究纳入 402 个治疗组和 15842 名参与者。在所有研究中,治疗组人数最多的是心理治疗(平均[标准差]人数,40.04 [36.88])和行为契约管理方案(平均[标准差]人数,37.51 [25.51])。仅行为契约管理方案与可卡因检测结果为阴性的可能性增加显著相关(OR,2.13;95%CI,1.62-2.80),并且在所有敏感性分析中这一关联仍然显著。
在这项荟萃分析中,行为契约管理方案与成人可卡因使用减少相关。与这种治疗方式相一致的研究努力和政策可能会使积极使用可卡因的人受益,并减轻社会负担。