Molecular Imaging and Therapy Service, Department of Radiology, Memorial Sloan Kettering Cancer Center, 1275 York Ave, Box 77, New York, NY, 10065, USA.
Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Eur J Nucl Med Mol Imaging. 2021 Nov;48(12):3940-3950. doi: 10.1007/s00259-021-05386-0. Epub 2021 May 8.
Current clinical and imaging tools remain suboptimal for predicting treatment response and prognosis in CNS lymphomas. We investigated the prognostic value of baseline [F]FDG PET in patients with CNS lymphoma receiving ibrutinib-based treatments.
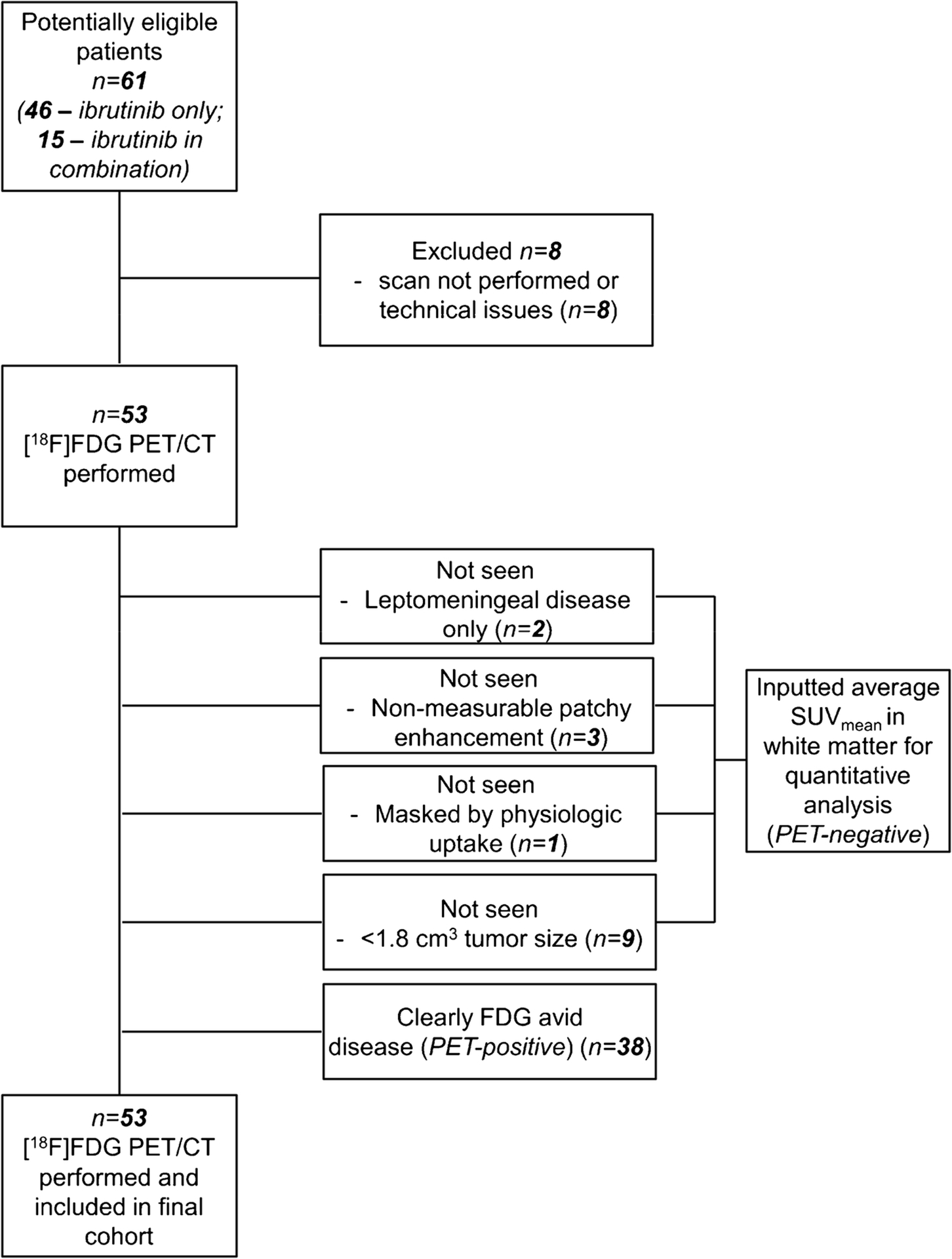
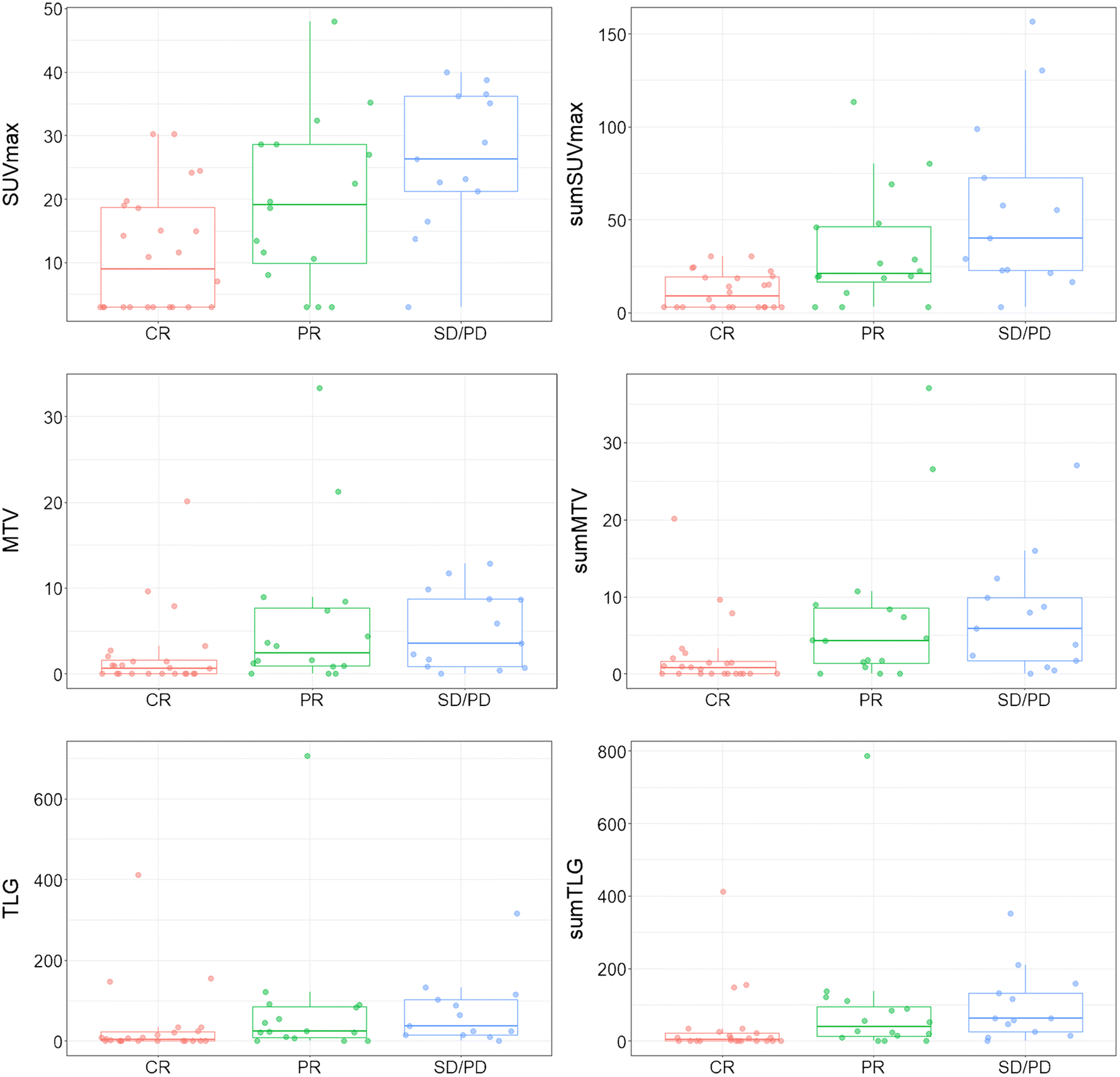
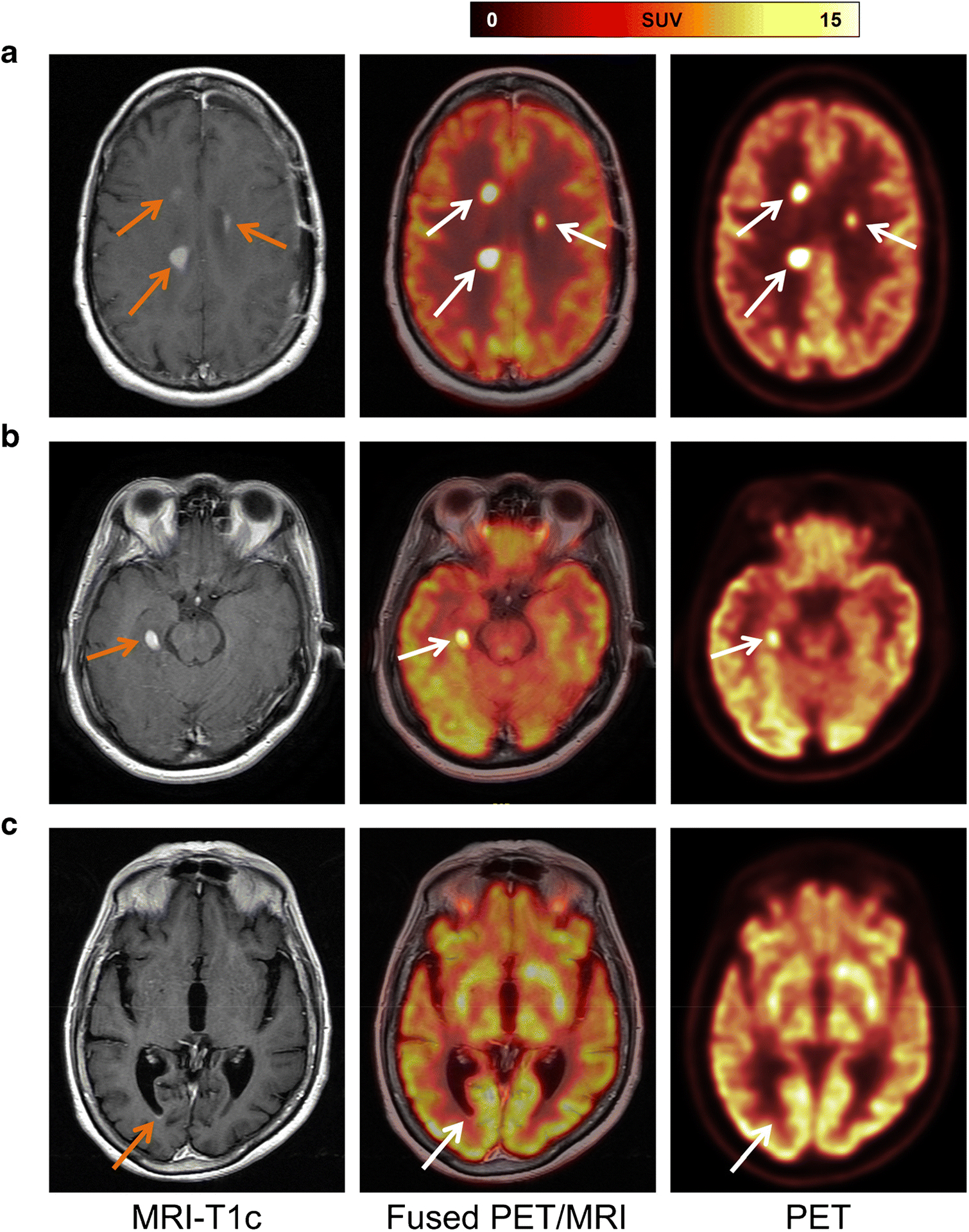
Fifty-three patients enrolled in a prospective clinical trial and underwent brain PET before receiving single-agent ibrutinib or ibrutinib in combination with methotrexate with or without rituximab. [F]FDG uptake in these lesions was quantified by drawing PET volumes of interest around up to five [F]FDG-avid lesions per patient (with uptake greater than surrounding brain). We measured standardized uptake values (SUV), metabolic tumor volumes, total lesion glycolysis (TLG), and the sum thereof in these lesions. We analyzed the relationship between PET parameters and mutation status, overall response rates, and progression-free survival (PFS).
Thirty-eight patients underwent single-agent therapy and 15 received combination therapy. On PET, 15/53 patients had no measurable disease. In the other 38 patients, a total of 71 lesions were identified on PET. High-intensity [F]FDG uptake and a larger volume of [F]FDG-avid disease were inversely related to treatment outcome (p ≤ 0.005). In univariable analysis, PFS was linearly correlated with all PET parameters, with stronger association when sum-values were used. A multivariable model showed that risk of progression increased by 9% for every 5-unit increase in sumSUV (hazard ratio = 1.09 [95% CI: 1.04 to 1.14]).
Higher lesional metabolic parameters are inversely related to outcome in patients undergoing ibrutinib-based therapies, and sumSUV emerged as a strong independent prognostic factor.
NCT02315326; https://clinicaltrials.gov/ct2/show/NCT02315326?term=NCT02315326&draw=2&rank=1.
目前的临床和影像学工具在预测中枢神经系统淋巴瘤的治疗反应和预后方面仍不尽如人意。我们研究了基线 [F]FDG PET 在接受伊布替尼为基础治疗的中枢神经系统淋巴瘤患者中的预后价值。
53 名患者入组一项前瞻性临床试验,在接受单药伊布替尼或伊布替尼联合甲氨蝶呤联合或不联合利妥昔单抗治疗前,进行脑部 PET 检查。通过对每位患者最多 5 个 [F]FDG 阳性病变(摄取大于周围脑)绘制 PET 感兴趣区,对这些病变的 [F]FDG 摄取进行定量。我们测量了标准化摄取值(SUV)、代谢肿瘤体积、总病灶糖酵解(TLG)和这些病灶的总和。我们分析了 PET 参数与突变状态、总缓解率和无进展生存期(PFS)之间的关系。
38 名患者接受单药治疗,15 名患者接受联合治疗。在 PET 上,53 名患者中有 15 名患者无可测量的疾病。在其他 38 名患者中,共在 PET 上发现 71 个病变。高强度 [F]FDG 摄取和更大的 [F]FDG 阳性病变体积与治疗结果呈负相关(p≤0.005)。在单变量分析中,PFS 与所有 PET 参数呈线性相关,当使用总和值时相关性更强。多变量模型显示,总和 SUV 每增加 5 个单位,进展的风险就会增加 9%(风险比=1.09 [95%CI:1.04 至 1.14])。
在接受伊布替尼为基础治疗的患者中,病变代谢参数越高,与预后呈负相关,而总和 SUV 则成为一个强有力的独立预后因素。
NCT02315326;https://clinicaltrials.gov/ct2/show/NCT02315326?term=NCT02315326&draw=2&rank=1。