Hifumi Toru, Inoue Akihiko, Takiguchi Toru, Watanabe Kazuhiro, Ogura Takayuki, Okazaki Tomoya, Ijuin Shinichi, Zushi Ryosuke, Arimoto Hideki, Takada Hiroaki, Shiraishi Shinichirou, Egawa Yuko, Kanda Jun, Nasu Michitaka, Kobayashi Makoto, Sakuraya Masaaki, Naito Hiromichi, Nakao Shunichiro, Otani Norio, Takeuchi Ichiro, Bunya Naofumi, Shimizu Takafumi, Sawano Hirotaka, Takayama Wataru, Kushimoto Shigeki, Shoko Tomohisa, Aoki Makoto, Otani Takayuki, Matsuoka Yoshinori, Homma Koichiro, Maekawa Kunihiko, Tahara Yoshio, Fukuda Reo, Kikuchi Migaku, Nakagami Takuo, Hagiwara Yoshihiro, Kitamura Nobuya, Sugiyama Kazuhiro, Sakamoto Tetsuya, Kuroda Yasuhiro
Department of Emergency and Critical Care Medicine St. Luke's International Hospital Tokyo Japan.
Department of Emergency and Critical Care Medicine Hyogo Emergency Medical Center Kobe Japan.
Acute Med Surg. 2021 May 1;8(1):e647. doi: 10.1002/ams2.647. eCollection 2021 Jan-Dec.
A lack of known guidelines for the provision of extracorporeal cardiopulmonary resuscitation (ECPR) to patients with out-of-hospital cardiac arrest (OHCA) has led to variability in practice between hospitals even in the same country. Because variability in ECPR practice has not been completely examined, we aimed to describe the variability in ECPR practice in patients with OHCA from the emergency department (ED) to the intensive care units (ICU).
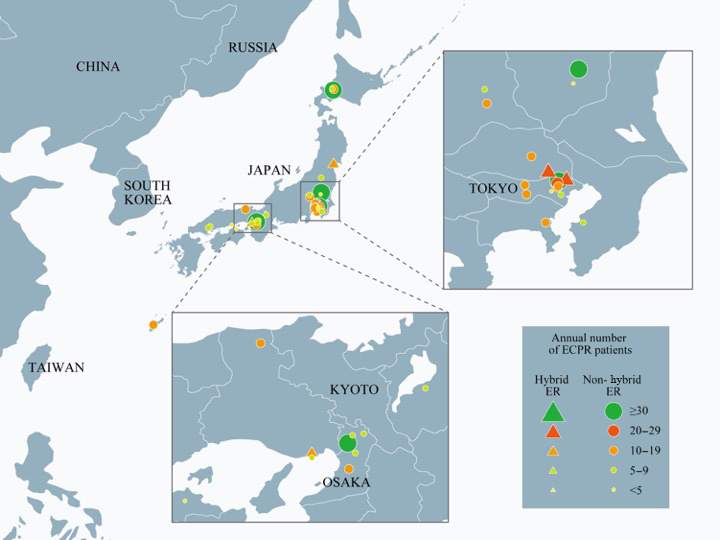
An anonymous online questionnaire to examine variability in ECPR practice was completed in January 2020 by 36 medical institutions who participated in the SAVE-J II study. Institutional demographics, inclusion and exclusion criteria, initial resuscitation management, extracorporeal membrane oxygenation (ECMO) initiation, initial ECMO management, intra-aortic balloon pumping/endotracheal intubation/management during coronary angiography, and computed tomography criteria were recorded.
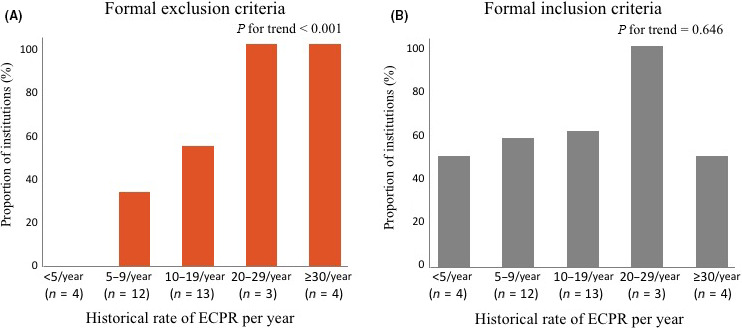
We received responses from all 36 institutions. Four institutions (11.1%) had a hybrid emergency room. Cardiovascular surgery was always involved throughout the entire ECMO process in only 14.7% of institutions; 60% of institutions had formal inclusion criteria and 50% had formal exclusion criteria. In two-thirds of institutions, emergency physicians carried out cannulation. Catheterization room was the leading location of cannulation (48.6%) followed by ED (31.4%). The presence of formal exclusion criteria significantly increased with increasing ECPR volume ( for trend <0.001). Intra-aortic balloon pumping was routinely initiated in only 25% of institutions. Computed tomography was routinely carried out before coronary angiography in 25% of institutions.
We described the variability in ECPR practice in patients with OHCA from the ED to the ICU.
由于缺乏针对院外心脏骤停(OHCA)患者进行体外心肺复苏(ECPR)的已知指南,即使在同一国家,不同医院的实践也存在差异。由于ECPR实践的差异尚未得到全面研究,我们旨在描述从急诊科(ED)到重症监护病房(ICU)的OHCA患者在ECPR实践中的差异。
2020年1月,参与SAVE-J II研究的36家医疗机构完成了一份用于调查ECPR实践差异的匿名在线问卷。记录了机构人口统计学、纳入和排除标准、初始复苏管理、体外膜肺氧合(ECMO)启动、初始ECMO管理、冠状动脉造影期间的主动脉内球囊泵入/气管插管/管理以及计算机断层扫描标准。
我们收到了所有36家机构的回复。4家机构(11.1%)设有混合急诊室。仅14.7%的机构在整个ECMO过程中始终有心血管外科参与;60%的机构有正式的纳入标准,50%有正式的排除标准。在三分之二的机构中,急诊医生进行插管操作。导管室是插管的主要地点(48.6%),其次是急诊科(31.4%)。随着ECPR量的增加,正式排除标准的存在显著增加(趋势检验P<0.001)。仅25%的机构常规启动主动脉内球囊泵入。25%的机构在冠状动脉造影前常规进行计算机断层扫描。
我们描述了从ED到ICU的OHCA患者在ECPR实践中的差异。