Department of Global Pediatric Medicine, St Jude Children's Research Hospital, Memphis, TN.
Department of Pediatrics, Division of Pediatric Hematology/Oncology, University of California San Diego, La Jolla, CA.
JCO Glob Oncol. 2021 May;7:659-670. doi: 10.1200/GO.20.00578.
Time to antibiotic administration (TTA) is a commonly used standard of care in pediatric cancer settings in high-income countries. Effective interventions to improve outcomes in cancer patients with febrile neutropenia (FN) often address timely and appropriate antibiotic administration. We assessed the effectiveness of a locally adapted multimodal strategy in decreasing TTA in a resource-constrained pediatric cancer center in Mexico.
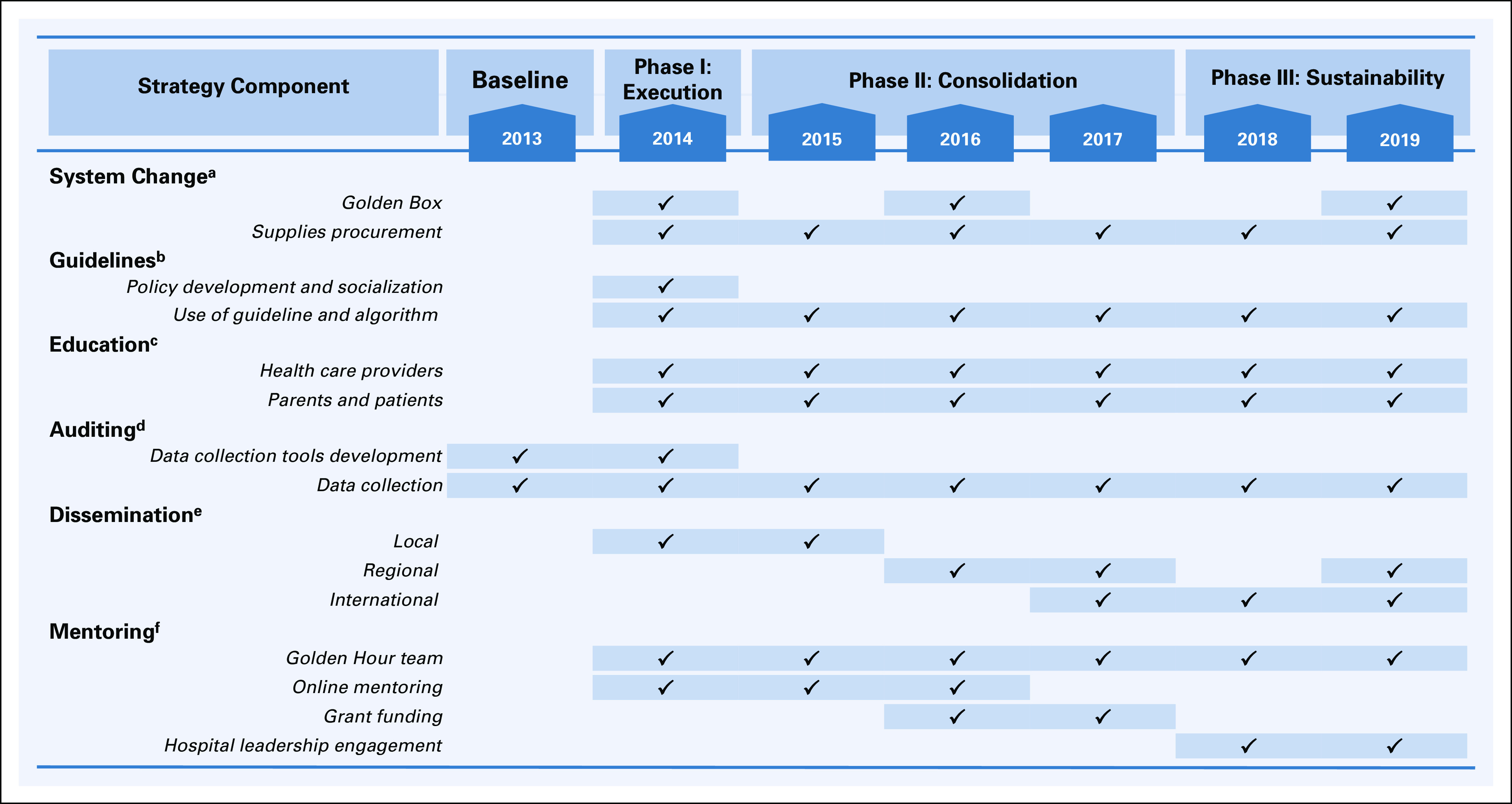
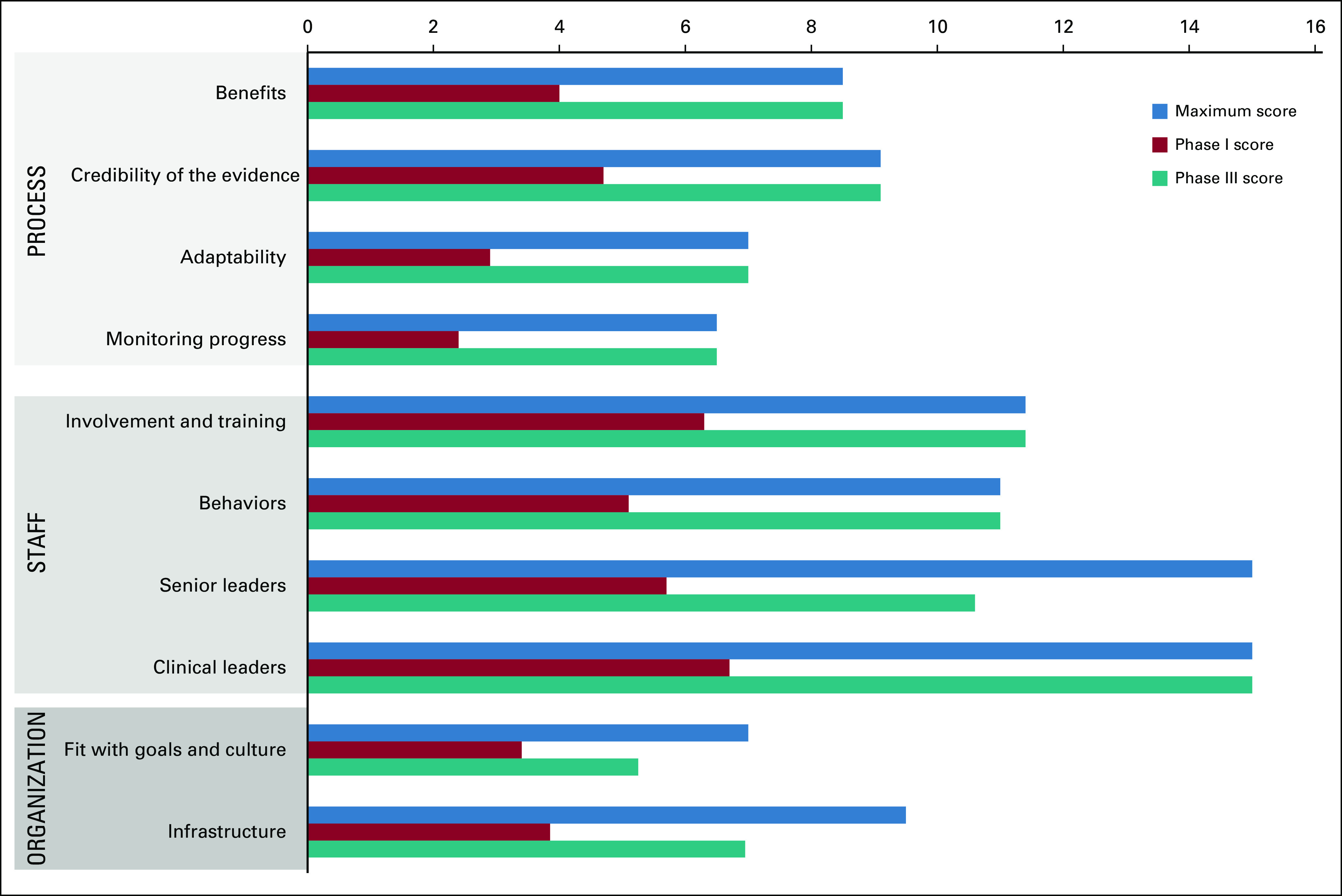
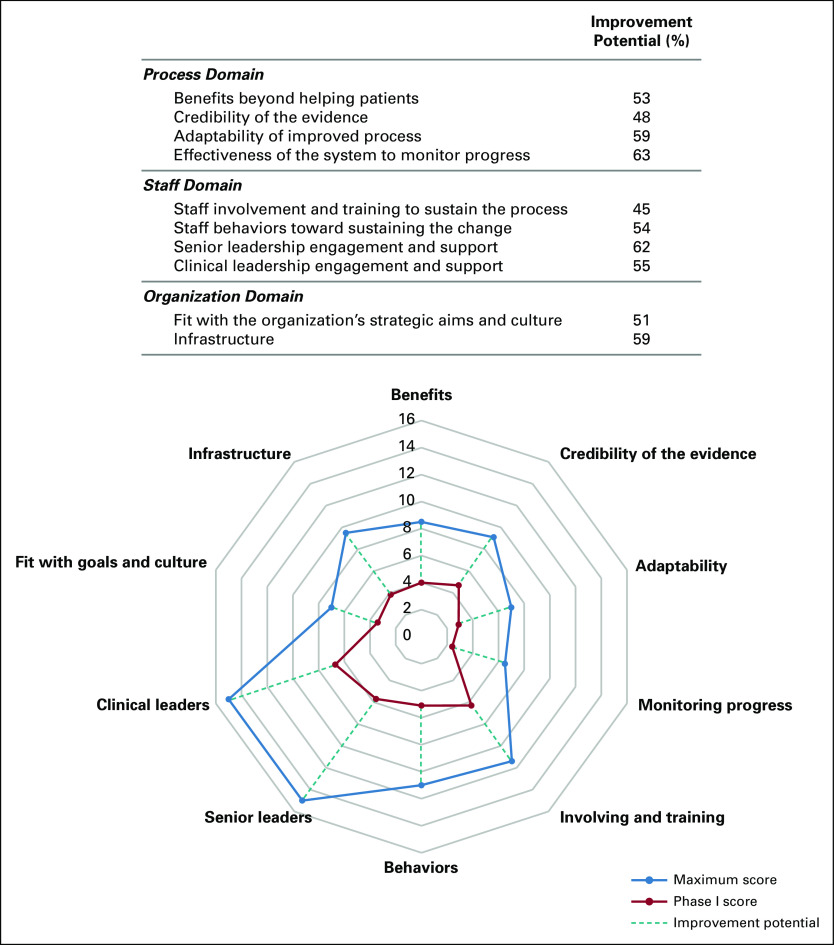
We conducted a prospective observational study between January 2014 and April 2019. A three-phase (phase I: execution, phase II: consolidation, phase III: sustainability) multimodal improvement strategy that combined system change, FN guideline development, education, auditing and monitoring, mentoring, and dissemination was implemented to decrease TTA in inpatient and ambulatory areas. Sustainability factors were measured by using a validated tool during phases I and III.
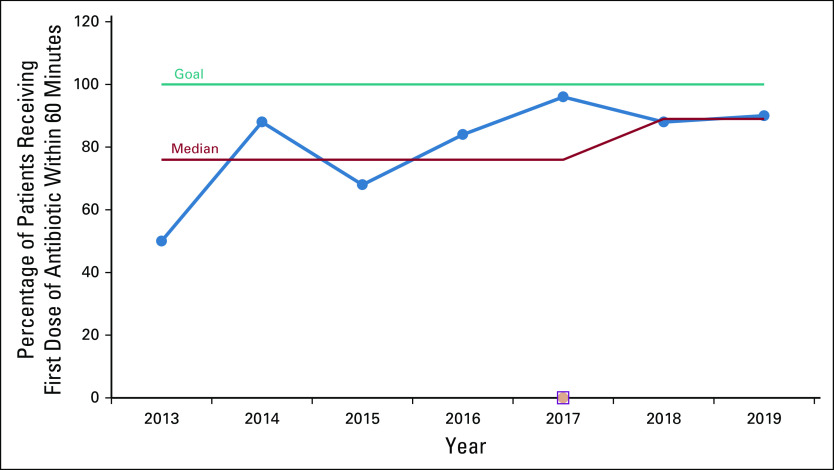
Our population included 105 children with cancer with 204 FN events. The baseline assessment revealed that only 50% of patients received antibiotics within 60 minutes of prescription (median time: inpatient, 75 minutes; ambulatory, 65 minutes). After implementing our improvement strategy, the percentage of patients receiving antibiotics within 60 minutes of prescription increased to 88%. We significantly decreased median TTA in both clinical areas during the three phases of the study. In phase III (sustainability), the median TTA was 40 minutes ( = .023) in the inpatient area and 30 minutes ( = .012) in the ambulatory area. The proportion of patients with sepsis decreased from 30% (baseline) to 5% (phase III) ( = .001).
Our results demonstrate that locally adapted multimodal interventions can reduce TTA in resource-constrained settings. Mentoring and dissemination were novel components of the multimodal strategy to improve FN-associated clinical outcomes. Improving local infrastructure, ongoing monitoring systems, and leadership engagement have been key factors to achieving sustainability during the 5-year period.
抗生素给药时间(TTA)是高收入国家儿科癌症环境中常用的护理标准。改善发热性中性粒细胞减少症(FN)癌症患者结局的有效干预措施通常涉及及时和适当的抗生素给药。我们评估了在墨西哥资源有限的儿科癌症中心中,对当地适应性的多模式策略在减少 TTA 方面的效果。
我们在 2014 年 1 月至 2019 年 4 月期间进行了一项前瞻性观察性研究。采用三阶段(阶段 I:执行,阶段 II:巩固,阶段 III:可持续性)多模式改进策略,该策略结合了系统变革、FN 指南制定、教育、审核和监测、指导以及传播,以减少住院和门诊区域的 TTA。在阶段 I 和 III 期间,使用经过验证的工具来衡量可持续性因素。
我们的人群包括 105 例患有癌症的儿童和 204 例 FN 事件。基线评估显示,只有 50%的患者在处方后 60 分钟内接受抗生素治疗(中位数时间:住院,75 分钟;门诊,65 分钟)。在实施我们的改进策略后,在处方后 60 分钟内接受抗生素治疗的患者比例增加到 88%。我们在研究的三个阶段均显著缩短了两个临床区域的 TTA 中位数。在第 III 阶段(可持续性),住院区域的 TTA 中位数为 40 分钟(P =.023),门诊区域为 30 分钟(P =.012)。败血症患者的比例从 30%(基线)下降到 5%(第 III 阶段)(P =.001)。
我们的结果表明,在资源有限的环境中,当地适应性的多模式干预措施可以缩短 TTA。指导和传播是改进 FN 相关临床结局的多模式策略中的新组成部分。改善当地基础设施、持续监测系统和领导层参与是在 5 年内实现可持续性的关键因素。