Cohen Clay, King Amber, Lin Chee Paul, Friedman Gregory K, Monroe Kathy, Kutny Matthew
From the *Department of Pediatrics, School of Medicine, †Division of Pediatric Emergency Medicine, Department of Pediatrics, ‡Center for Clinical and Translational Science, §Division of Pediatric Hematology/Oncology, Department of Pediatrics, University of Alabama at Birmingham, Birmingham, AL.
Pediatr Emerg Care. 2016 Nov;32(11):739-745. doi: 10.1097/PEC.0000000000000362.
Patients with febrile neutropenia are at high risk of morbidity and mortality from infectious causes. Decreasing time to antibiotic (TTA) administration is associated with improved patient outcomes. We sought to reduce TTA for children presenting to the emergency department with fever and neutropenia.
In a prospective cohort study with historical comparison, TTA administration was evaluated in patients with neutropenia presenting to the Children's of Alabama Emergency Department. A protocol was established to reduce delays in antibiotic administration and increase the percentage of patients who receive treatment within 60 minutes of presentation. One hundred pre-protocol patient visits between August 2010 and December 2011 were evaluated and 153 post-protocol visits were evaluated between August 2012 and September 2013. We reviewed individual cases to determine barriers to rapid antibiotic administration.
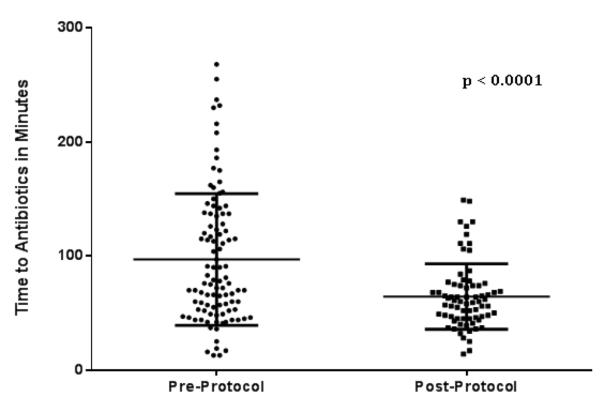
Antibiotics were administered in 96.9 ± 57.8 minutes in the pre-protocol patient group, and only 35% of patients received antibiotics within 60 minutes of presentation and 70% received antibiotics within 120 minutes. After implementation of the protocol, TTA for neutropenic patients was decreased to 64.3 ± 28.4 minutes (P < 0.0001) with 51.4% receiving antibiotics within 60 minutes and 93.2% within 120 minutes.
Implementing a standard approach to patients at risk for neutropenia decreased TTA. There are numerous challenges in providing timely antibiotics to children with febrile neutropenia. Identified delays included venous access (time to effect of topical anesthetics, and difficulty obtaining access), physicians waiting on laboratory results, and antibiotic availability.
发热性中性粒细胞减少症患者因感染原因导致发病和死亡的风险很高。缩短抗生素给药时间(TTA)与改善患者预后相关。我们试图缩短因发热和中性粒细胞减少症就诊于急诊科的儿童的TTA。
在一项进行历史对照的前瞻性队列研究中,对就诊于阿拉巴马州儿童医院急诊科的中性粒细胞减少症患者的TTA进行了评估。制定了一项方案以减少抗生素给药延迟,并提高在就诊后60分钟内接受治疗的患者比例。对2010年8月至2011年12月期间100例方案实施前的患者就诊情况进行了评估,对2012年8月至2013年9月期间153例方案实施后的就诊情况进行了评估。我们审查了个体病例以确定快速给予抗生素的障碍。
方案实施前患者组抗生素给药时间为96.9±57.8分钟,只有35%的患者在就诊后60分钟内接受抗生素治疗,70%的患者在120分钟内接受治疗。实施该方案后,中性粒细胞减少症患者的TTA降至64.3±28.4分钟(P<0.0001),51.4%的患者在60分钟内接受抗生素治疗,93.2%的患者在120分钟内接受治疗。
对有中性粒细胞减少症风险的患者实施标准化方法可缩短TTA。为发热性中性粒细胞减少症儿童及时提供抗生素存在诸多挑战。已确定的延迟包括静脉通路(局部麻醉起效时间和难以获得通路)、医生等待实验室结果以及抗生素可用性。