Department of Surgical Oncology, CRCM, Institut Paoli-Calmettes, Aix-Marseille Univ, CNRS, INSERM, Marseille, France.
Department of Medical Oncology, CRCM, Institut Paoli-Calmettes, Aix-Marseille Univ, CNRS, INSERM, Marseille, France.
ESMO Open. 2021 Jun;6(3):100151. doi: 10.1016/j.esmoop.2021.100151. Epub 2021 May 10.
Prognostic impact of lymph node micro-metastases (pN1mi) has been discordantly reported in the literature. The need to clarify this point for decision-making regarding adjuvant therapy, particularly for patients with endocrine receptor (ER)-positive status and HER2-negative tumors, is further reinforced by the generalization of gene expression signatures using pN status in their recommendation algorithm.
We retrospectively analyzed 13 773 patients treated for ER-positive breast cancer in 13 French cancer centers from 1999 to 2014. Five categories of axillary lymph node (LN) status were defined: negative LN (pN0i-), isolated tumor cells [pN0(i+)], pN1mi, and pN1 divided into single (pN1 = 1) and multiple (pN1 > 1) macro-metastases (>2 mm). The effect of LN micro-metastases on outcomes was investigated both in the entire cohort of patients and in clinically relevant subgroups according to tumor subtypes. Propensity-score-based matching was used to balance differences in known prognostic variables associated with pN status.
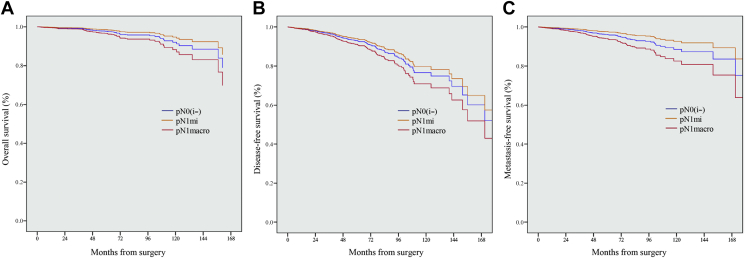
As determined by sentinel LN biopsy, 9427 patients were pN0 (68.4%), 546 pN0(i+) (4.0%), 1446 pN1mi (10.5%) and 2354 pN1 with macro-metastases (17.1%). With a median follow-up of 61.25 months, pN1 status, but not pN1mi, significantly impacted overall survival (OS), disease-free survival (DFS), metastasis-free survival (MFS), and breast-cancer-specific survival. In the subgroup of patients with known tumor subtype, pN1 = 1, as pN1 > 1, but not pN1mi, had a significant prognostic impact on OS. DFS and MFS were only impacted by pN1 > 1. Similar results were observed in the subgroup of patients with luminal A-like tumors (n = 7101). In the matched population analysis, pN1macro, but not pN1mi, had a statistically significant negative impact on MFS and OS.
LN micro-metastases have no detectable prognostic impact and should not be considered as a determining factor in indicating adjuvant chemotherapy. The evaluation of the risk of recurrence using second-generation signatures should be calculated considering micro-metastases as pN0.
淋巴结微转移(pN1mi)的预后影响在文献中存在争议。对于需要辅助治疗的患者,特别是对于内分泌受体(ER)阳性状态和 HER2 阴性肿瘤患者,需要明确这一点,因为基因表达谱的泛化在其推荐算法中使用了 pN 状态。
我们回顾性分析了 1999 年至 2014 年 13 个法国癌症中心治疗的 13773 例 ER 阳性乳腺癌患者。定义了 5 类腋窝淋巴结(LN)状态:阴性 LN(pN0i-)、孤立肿瘤细胞[pN0(i+)]、pN1mi 和 pN1 分为单(pN1=1)和多(pN1>1)个宏转移(>2mm)。根据肿瘤亚型,在整个患者队列和临床相关亚组中研究了 LN 微转移对结局的影响。采用倾向评分匹配来平衡与 pN 状态相关的已知预后变量的差异。
通过前哨淋巴结活检确定,9427 例患者为 pN0(68.4%),546 例 pN0(i+)(4.0%),1446 例 pN1mi(10.5%)和 2354 例 pN1 有宏转移(17.1%)。中位随访 61.25 个月后,pN1 状态但不是 pN1mi 显著影响总生存期(OS)、无病生存期(DFS)、无转移生存期(MFS)和乳腺癌特异性生存期。在已知肿瘤亚型的患者亚组中,pN1=1(与 pN1>1 一样),但不是 pN1mi,对 OS 有显著的预后影响。DFS 和 MFS 仅受 pN1>1 的影响。在 luminal A 样肿瘤(n=7101)的亚组中观察到类似的结果。在匹配人群分析中,pN1macro,但不是 pN1mi,对 MFS 和 OS 有统计学上显著的负面影响。
LN 微转移没有可检测到的预后影响,不应被视为指示辅助化疗的决定因素。使用第二代标志物评估复发风险时,应将微转移视为 pN0 进行计算。