Kuo Ming-Jen, Chou Ruey-Hsing, Lu Ya-Wen, Guo Jiun-Yu, Tsai Yi-Lin, Wu Cheng-Hsueh, Huang Po-Hsun, Lin Shing-Jong
Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
Cardiovascular Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan.
J Intensive Care. 2021 May 13;9(1):40. doi: 10.1186/s40560-021-00553-9.
β-blockers may protect against catecholaminergic myocardial injury in critically ill patients. Long-term β-blocker users are known to have lower lactate concentrations and favorable sepsis outcomes. However, the effects of β1-selective and nonselective β-blockers on sepsis outcomes have not been compared. This study was conducted to investigate the impacts of different β-blocker classes on the mortality rate in septic patients.
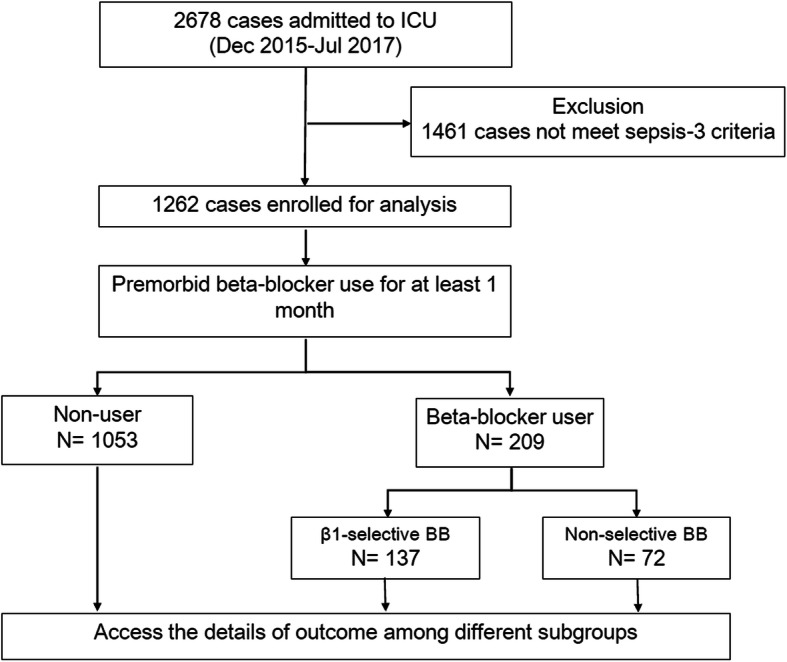
We retrospectively screened 2678 patients admitted to the medical or surgical intensive care unit (ICU) between December 2015 and July 2017. Data from patients who met the Sepsis-3 criteria at ICU admission were included in the analysis. Premorbid β-blocker exposure was defined as the prescription of any β-blocker for at least 1 month. Bisoprolol, metoprolol, and atenolol were classified as β1-selective β-blockers, and others were classified as nonselective β-blockers. All patients were followed for 28 days or until death.
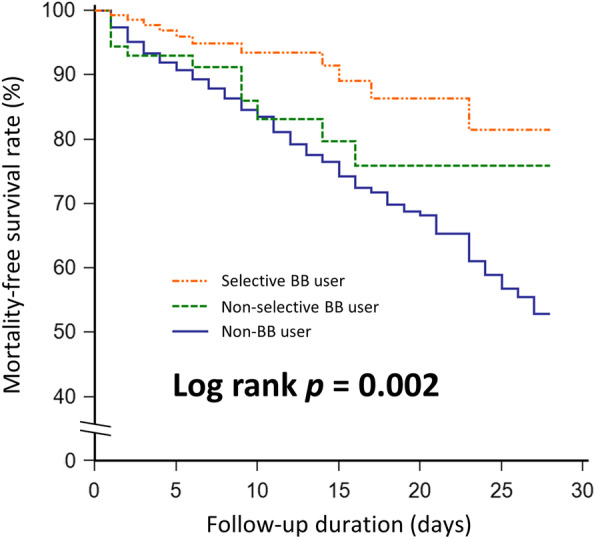
Among 1262 septic patients, 209 (16.6%) patients were long-term β-blocker users. Patients with premorbid β-blocker exposure had lower heart rates, initial lactate concentrations, and ICU mortality. After adjustment for disease severity, comorbidities, blood pressure, heart rate, and laboratory data, reduced ICU mortality was associated with premorbid β1-selective [adjusted hazard ratio, 0.40; 95% confidence interval (CI), 0.18-0.92; P = 0.030], but not non-selective β-blocker use.
Premorbid β1-selective, but not non-selective, β-blocker use was associated with improved mortality in septic patients. This finding supports the protective effect of β1-selective β-blockers in septic patients. Prospective studies are needed to confirm it.
β受体阻滞剂可能对危重症患者儿茶酚胺能性心肌损伤起到保护作用。已知长期使用β受体阻滞剂的患者乳酸浓度较低,脓毒症预后较好。然而,β1选择性和非选择性β受体阻滞剂对脓毒症预后的影响尚未进行比较。本研究旨在调查不同类别β受体阻滞剂对脓毒症患者死亡率的影响。
我们回顾性筛选了2015年12月至2017年7月期间入住内科或外科重症监护病房(ICU)的2678例患者。分析纳入了在ICU入院时符合脓毒症-3标准的患者数据。病前β受体阻滞剂暴露定义为服用任何β受体阻滞剂至少1个月。比索洛尔、美托洛尔和阿替洛尔被归类为β1选择性β受体阻滞剂,其他则归类为非选择性β受体阻滞剂。所有患者随访28天或直至死亡。
在1262例脓毒症患者中,209例(16.6%)为长期β受体阻滞剂使用者。病前暴露于β受体阻滞剂的患者心率、初始乳酸浓度和ICU死亡率较低。在调整疾病严重程度、合并症、血压、心率和实验室数据后,ICU死亡率降低与病前使用β1选择性β受体阻滞剂相关[调整后风险比,0.40;95%置信区间(CI),0.18 - 0.92;P = 0.030],但与使用非选择性β受体阻滞剂无关。
病前使用β1选择性而非非选择性β受体阻滞剂与脓毒症患者死亡率改善相关。这一发现支持了β1选择性β受体阻滞剂对脓毒症患者的保护作用。需要前瞻性研究来证实这一点。