Department of Cardiac, Thoracic and Vascular Surgery, Odense University Hospital, J. B. Winsløws Vej 4, 5000, Odense C, Denmark.
Faculty of Health Science, University of Southern Denmark, Odense, Denmark.
J Cardiothorac Surg. 2021 May 14;16(1):130. doi: 10.1186/s13019-021-01506-x.
This study describes the long-term survival, risk of reoperation and clinical outcomes of patients undergoing solitary surgical aortic valve replacement (SAVR) with a Carpentier-Edwards Perimount (CE-P) bioprosthetic in Western Denmark. The renewed interest in SAVR is based on the questioning regarding the long-term survival since new aortic replacement technique such as transcatheter aortic-valve replacement (TAVR) probably have shorter durability, why assessment of long-term survival could be a key issue for patients.
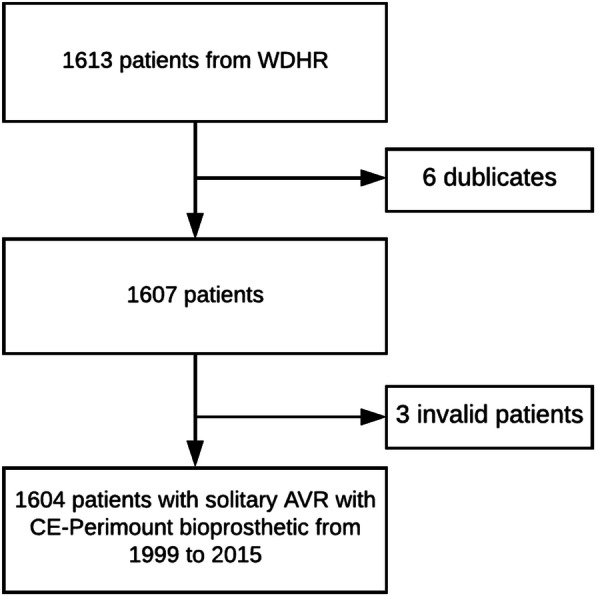
From November 1999 to November 2013 a cohort of a total of 1604 patients with a median age of 73 years (IQR: 69-78) undergoing solitary SAVR with CE-P in Western Denmark was obtained November 2018 from the Western Danish Heart Registry (WDHR). The primary endpoint was long-term survival from all-cause mortality. Secondary endpoints were survival free from major adverse cardiovascular and cerebral events (MACCE), risk of reoperation, cause of late death, patient-prothesis mismatch, risk of AMI, stroke, pacemaker or ICD implantation and postoperative atrial fibrillation (POAF). Time-to-event analysis was performed with Kaplan-Meier curve, cumulative incidence function was performed with Nelson-Aalen cumulative hazard estimates. Cox regression was applied to detect risk factors for death and reoperation.
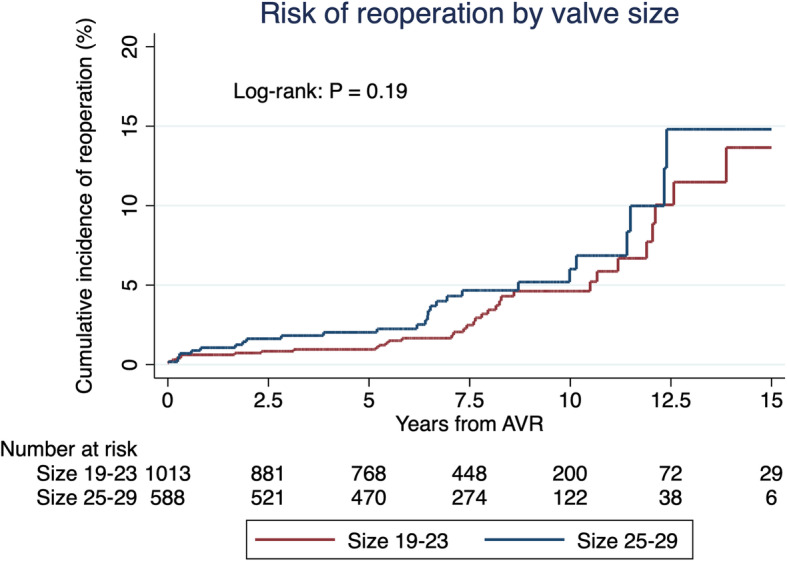
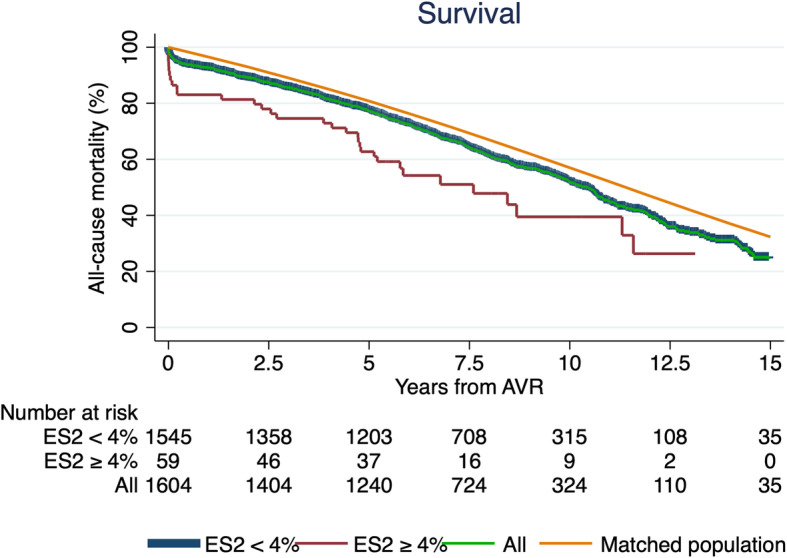
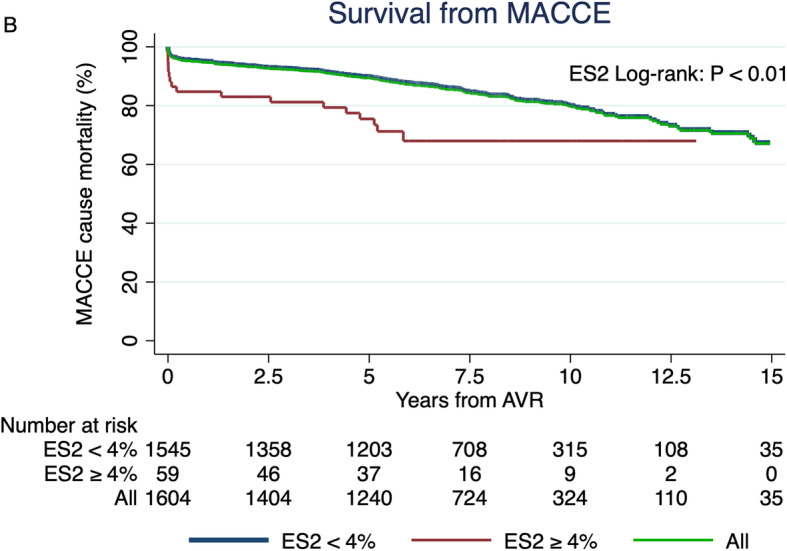
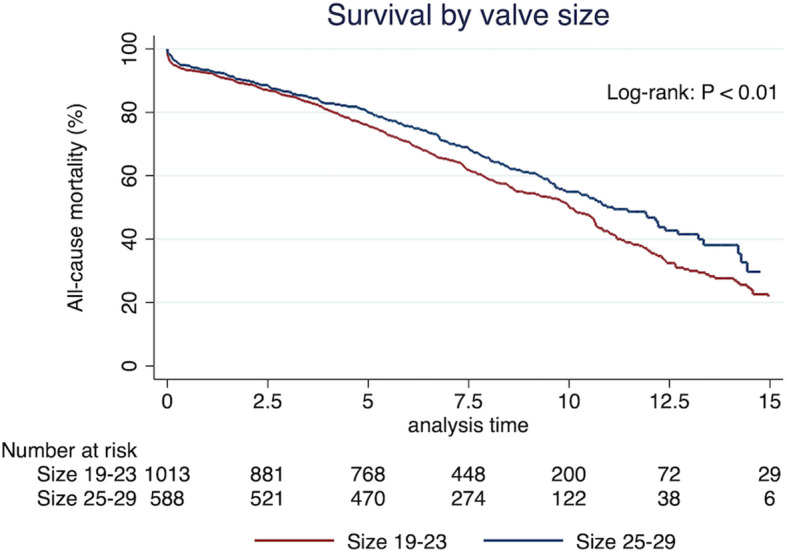
In-hospital mortality was 2.7% and 30-day mortality at 3.4%. The 5-, 10- and 15-year survival from all-cause mortality was 77, 52 and 24%, respectively. Survival without MACCE was 80% after 10 years. Significant risk factors of mortality were small valves, smoking and EuroSCORE II ≥4%. The risk of reoperation was < 5% after 7.5 years and significant risk factors were valve prosthesis-patient mismatch and EuroSCORE II ≥4%.
Patients undergoing aortic valve replacement with a Carpentier-Edwards Perimount valve shows a very satisfying long-term survival. Future research should aim to investigate biological valves long-term durability for comparison of different SAVR to different TAVR in long perspective.
本研究描述了在丹麦西部,接受单一外科主动脉瓣置换术(SAVR)并使用 Carpentier-Edwards Perimount(CE-P)生物瓣的患者的长期生存、再次手术风险和临床结果。对 SAVR 的重新关注基于对长期生存的质疑,因为新的主动脉置换技术(如经导管主动脉瓣置换术(TAVR))的耐久性可能较短,为什么评估长期生存可能是患者的关键问题。
从 1999 年 11 月到 2013 年 11 月,在丹麦西部,总共获得了 1604 名接受 CE-P 进行单一 SAVR 的患者队列,这些患者的中位年龄为 73 岁(IQR:69-78)。2018 年 11 月,从丹麦西部心脏注册处(WDHR)获得了这些患者的数据。主要终点是全因死亡率的长期生存。次要终点是无主要不良心血管和脑事件(MACCE)的生存、再次手术风险、晚期死亡原因、患者-假体不匹配、急性心肌梗死(AMI)、中风、起搏器或 ICD 植入和术后心房颤动(POAF)风险。使用 Kaplan-Meier 曲线进行时间事件分析,使用 Nelson-Aalen 累积风险估计进行累积发生率函数分析。Cox 回归用于检测死亡和再次手术的风险因素。
住院死亡率为 2.7%,30 天死亡率为 3.4%。全因死亡率的 5 年、10 年和 15 年生存率分别为 77%、52%和 24%。10 年后无 MACCE 的生存率为 80%。死亡率的显著危险因素是小瓣膜、吸烟和 EuroSCORE II≥4%。7.5 年后再次手术的风险<5%,显著的危险因素是瓣膜假体-患者不匹配和 EuroSCORE II≥4%。
接受 Carpentier-Edwards Perimount 瓣膜主动脉瓣置换术的患者具有非常满意的长期生存率。未来的研究应旨在调查生物瓣膜的长期耐久性,以便在长期视角下比较不同的 SAVR 和不同的 TAVR。