Internal Department C, affiliated with the Sackler Faculty of Medicine, Yitzhak Shamir Medical Center, Tel Aviv University, Zerifin, Israel.
Nephrology Division, affiliated with the Sackler Faculty of Medicine, Tel Aviv University, Yitzhak Shamir Medical Center, 70300, Zerifin, Israel.
BMC Nephrol. 2021 May 15;22(1):179. doi: 10.1186/s12882-021-02384-0.
We tested whether CHADS-VASc and/or HAS-BLED scores better predict ischemic stroke and major bleeding, respectively, than their individual components in maintenance hemodialysis (MHD) patients with atrial fibrillation (AF).
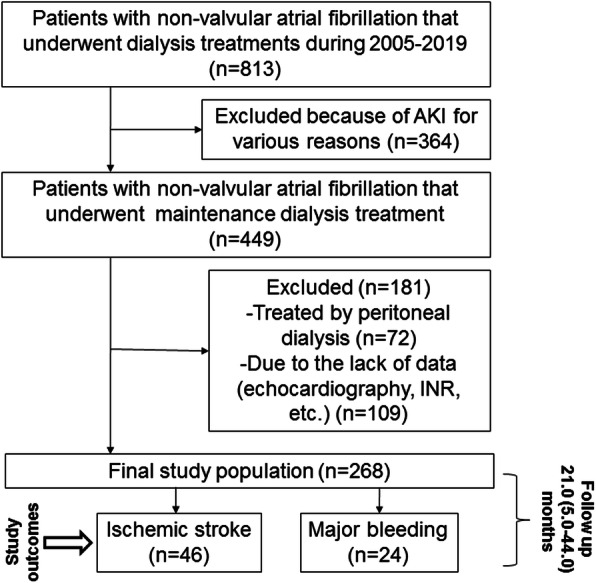
A retrospective cohort study of a clinical database containing the medical records of 268 MHD patients with non-valvular AF (167 women, mean age 73.4 ± 10.2 years). During the median follow-up of 21.0 (interquartile range, 5.0-44.0) months, 46 (17.2%) ischemic strokes and 24 (9.0%) major bleeding events were reported.
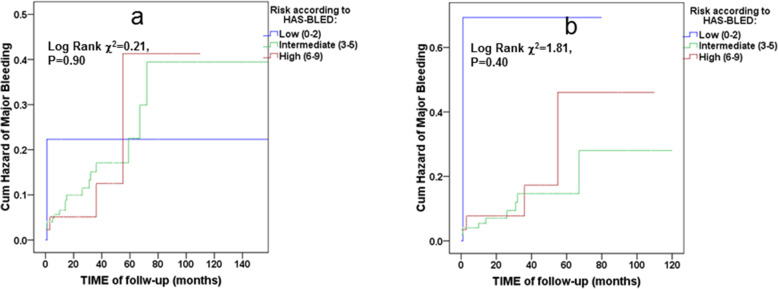
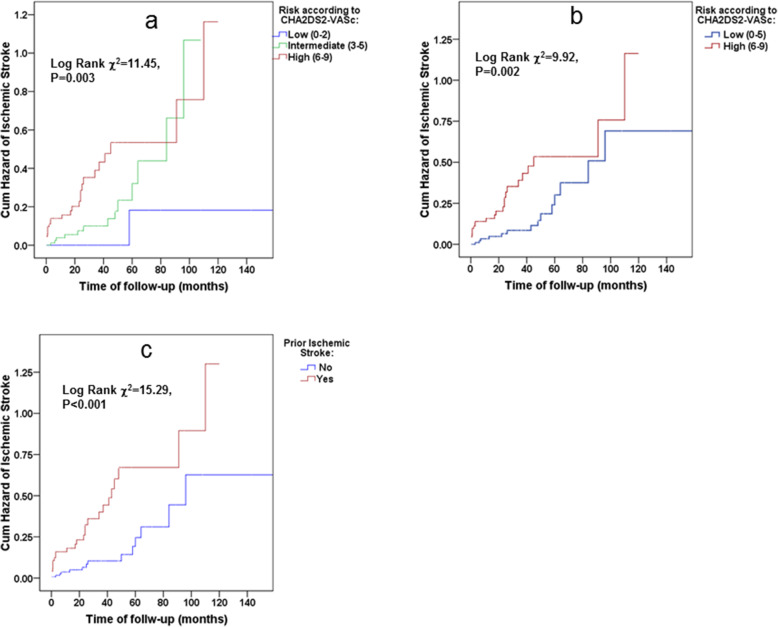
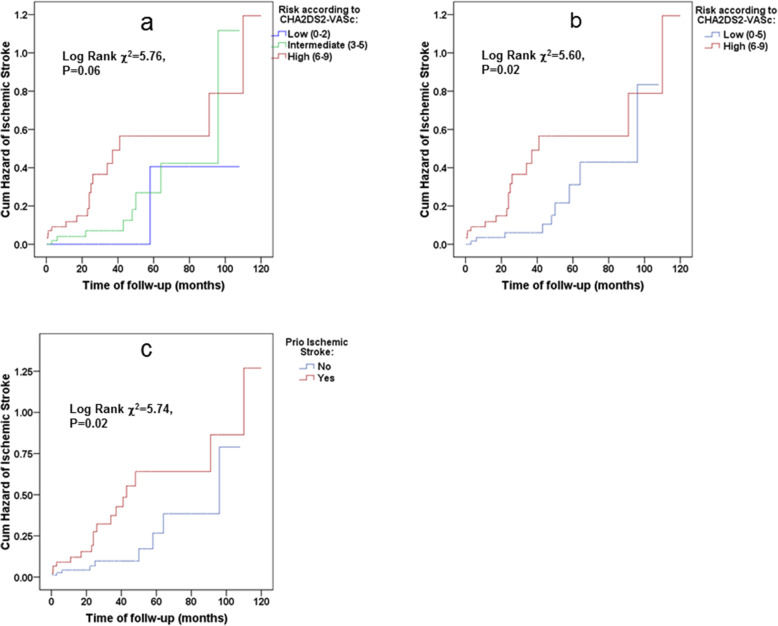
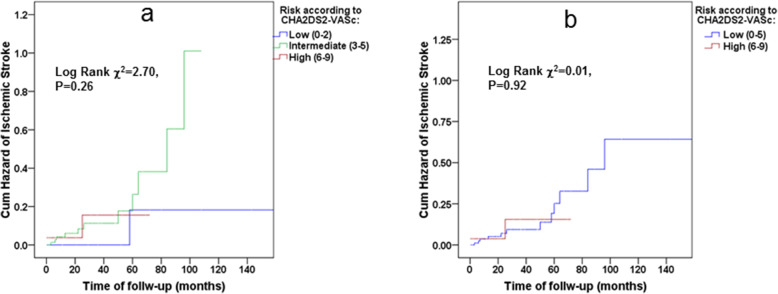
Although CHADS-VASc predicted ischemic stroke risk in the study population (adjusted HR 1.74 with 95% CI 1.23-2.46 for each unit of increase in CHADS-VASc score, and HR of 5.57 with 95% CI 1.88-16.49 for CHADS-VASc score ≥ 6), prior ischemic strokes/transient ischemic attacks (TIAs) were non-inferior in both univariate and multivariate analyses (adjusted HR 8.65 with 95% CI 2.82-26.49). The ROC AUC was larger for the prior ischemic stroke/TIA than for CHADS-VASc. Furthermore, the CHADS-VASc score did not predict future ischemic stroke risks in study participants who did not previously experience ischemic strokes/TIAs (adjusted HR 1.41, 95% CI: 0.84-2.36). The HAS-BLED score and its components did not have predictive abilities in discriminating bleeding risk in the study population.
Previous ischemic strokes are non-inferior for predicting of future ischemic strokes than the complete CHADS-VASc score in MHD patients. CHADSVASc scores are less predictive in MHD patients without histories of CVA/TIA. HAS-BLED scores do not predict major bleeding in MHD patients. These findings should redesign approaches to ischemic stroke risk stratification in MHD patients if future large-scale epidemiological studies confirm them.
我们测试了 CHADS-VASc 和/或 HAS-BLED 评分在预测维持性血液透析(MHD)合并心房颤动(AF)患者的缺血性卒中和主要出血方面,是否优于其各组成部分。
对包含 268 例非瓣膜性 AF 合并 MHD 患者(167 例女性,平均年龄 73.4±10.2 岁)的临床数据库进行回顾性队列研究。在中位随访 21.0(四分位间距 5.0-44.0)个月期间,报告了 46 例(17.2%)缺血性卒中和 24 例(9.0%)主要出血事件。
尽管 CHADS-VASc 预测了研究人群的缺血性卒中风险(每增加 1 分 CHADS-VASc 评分,调整后的 HR 为 1.74,95%CI 为 1.23-2.46,CHADS-VASc 评分≥6 时的 HR 为 5.57,95%CI 为 1.88-16.49),但既往缺血性卒中和短暂性脑缺血发作(TIA)在单变量和多变量分析中均无差异(调整后的 HR 为 8.65,95%CI 为 2.82-26.49)。与 CHADS-VASc 评分相比,既往缺血性卒中和 TIA 的 ROC AUC 更大。此外,CHADS-VASc 评分在既往无缺血性卒中和 TIA 病史的患者中,不能预测未来缺血性卒中风险(调整后的 HR 为 1.41,95%CI:0.84-2.36)。HAS-BLED 评分及其各组成部分在预测研究人群出血风险方面均无预测能力。
既往缺血性卒中和 TIA 在预测 MHD 患者未来缺血性卒中方面与完整的 CHADS-VASc 评分相当。在既往无 CVA/TIA 病史的 MHD 患者中,CHADSVASc 评分的预测能力较低。HAS-BLED 评分不能预测 MHD 患者的主要出血事件。如果未来的大规模流行病学研究证实这些发现,这些发现应重新设计 MHD 患者缺血性卒中风险分层方法。