Department of Neurosurgery, Stanford University School of Medicine, 300 Pasteur Drive, Palo Alto, CA 94305, USA.
California Northstate University College of Medicine, 9700 W Taron Drive, Elk Grove, CA 95757, USA; Department of Neurosurgery, Santa Clara Valley Medical Center, 751 S Bascom Ave, San Jose, CA 95128, USA.
J Clin Neurosci. 2021 Jun;88:128-134. doi: 10.1016/j.jocn.2021.03.017. Epub 2021 Apr 4.
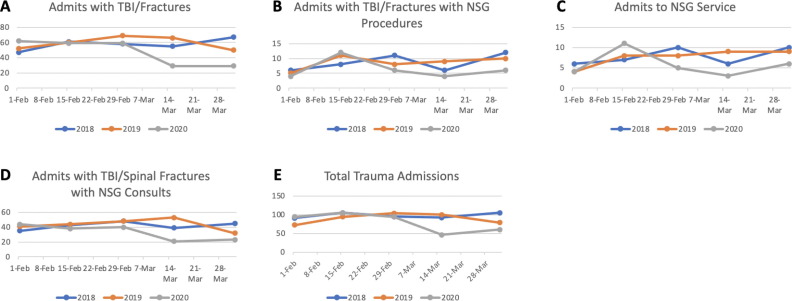
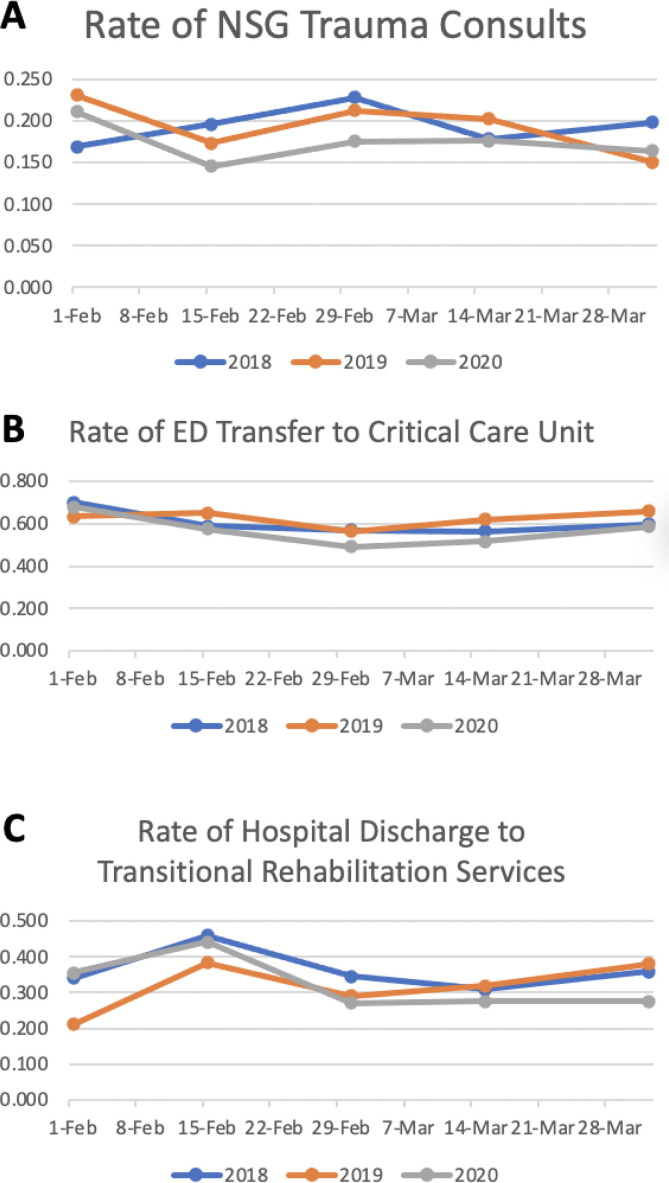
Early COVID-19-targeted legislations reduced public activity and elective surgery such that local neurosurgical care greatly focused on emergent needs. This study examines neurosurgical trauma patients' dispositions through two neighboring trauma centers to inform resource allocation. We conducted a retrospective review of the trauma registries for two Level 1 Trauma Centers in Santa Clara County, one academic and one community center, between February 1st and April 15th, 2018-2020. Events before a quarantine, implemented on March 16th, 2020, and events from 2018 to 19 were used for reference. Encounters were characterized by injuries, services, procedures, and disposition. Categorical variables were analyzed by the χ2 test, proportions of variables by z-score test, and non-parametric variables by Fisher's exact test. A total of 1,336 traumas were identified, with 31% from the academic center and 69% from the community center. During the post-policy period, relative to matching periods in years prior, there was a decrease in number of TBI and spinal fractures (24% versus 41%, p < 0.001) and neurosurgical consults (27% versus 39%, p < 0.003), but not in number of neurosurgical admissions or procedures. There were no changes in frequency of neurosurgery consults among total traumas, patients triaged to critical care services, or patients discharged to temporary rehabilitation services. Neurosurgical services were similarly rendered between the academic and community hospitals. This study describes neurosurgical trauma management in a suburban healthcare network immediately following restrictive quarantine during a moderate COVID-19 outbreak. Our data shows that neurosurgery remains a resource-intensive subspeciality, even during restrictive periods when overall trauma volume is decreased.
早期针对 COVID-19 的立法减少了公众活动和选择性手术,因此当地神经外科护理主要集中在紧急需求上。本研究通过两个相邻的创伤中心检查神经外科创伤患者的处置情况,以告知资源分配。我们对圣克拉拉县的两个 1 级创伤中心(一个学术中心和一个社区中心)的创伤登记处进行了回顾性研究,时间为 2018 年 2 月 1 日至 2020 年 4 月 15 日。参考了 2020 年 3 月 16 日实施的隔离政策之前的事件和 2018 年至 19 年的事件。事件特征包括损伤、服务、程序和处置。使用 χ2 检验分析分类变量,z 分数检验分析变量比例,Fisher 精确检验分析非参数变量。共确定了 1336 例创伤,其中 31%来自学术中心,69%来自社区中心。在政策后时期,与前几年的同期相比,TBI 和脊柱骨折的数量减少了(24%比 41%,p<0.001),神经外科会诊的数量减少了(27%比 39%,p<0.003),但神经外科入院或手术的数量没有增加。在总创伤、分诊至重症监护服务的患者或出院至临时康复服务的患者中,神经外科会诊的频率没有变化。学术和社区医院的神经外科服务相似。本研究描述了 COVID-19 中度爆发期间,在限制隔离期间,郊区医疗网络中神经外科创伤管理的情况。我们的数据表明,即使在总体创伤量减少的限制时期,神经外科仍然是资源密集型的亚专业。