Unluhizarci Kursad, Karaca Zuleyha, Kelestimur Fahrettin
Department of Endocrinology, Erciyes University Medical School, Kayseri, 38039, Turkey.
Department of Endocrinology, Yeditepe University Medical School, Istanbul, 34755, Turkey.
World J Diabetes. 2021 May 15;12(5):616-629. doi: 10.4239/wjd.v12.i5.616.
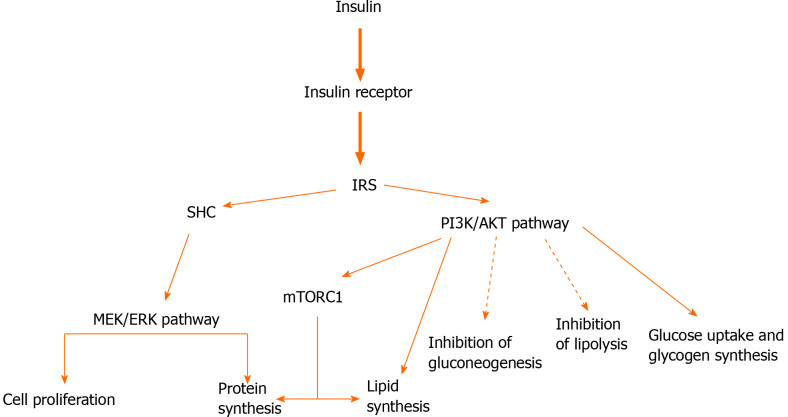
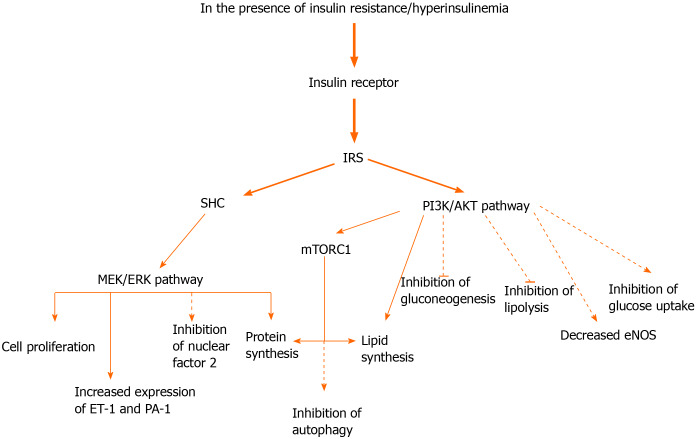
Insulin has complex effects on cell growth, metabolism and differentiation, and these effects are mediated by a cell-surface bound receptor and eventually a cascade of intracellular signaling events. Among the several metabolic and growth-promoting effects of insulin, insulin resistance is defined as an attenuated effect of insulin on glucose metabolism, primarily the limited export of blood glucose into skeletal muscle and adipose tissue. On the other hand, not all the signaling pathways and insulin-responsive tissues are equally affected, and some effects other than the metabolic actions of insulin are overexpressed. Ovaries and the adrenal glands are two examples of tissues remaining sensitive to insulin actions where insulin may contribute to increased androgen secretion. Polycystic ovary syndrome (PCOS) is the most common form of androgen excess disorder (AED), and its pathogenesis is closely associated with insulin resistance. Patients with idiopathic hirsutism also exhibit insulin resistance, albeit lower than patients with PCOS. Although it is not as evident as in PCOS, patients with congenital adrenal hyperplasia may have insulin resistance, which may be further exacerbated with glucocorticoid overtreatment and obesity. Among patients with severe insulin resistance syndromes, irrespective of the type of disease, hyperinsulinemia promotes ovarian androgen synthesis independently of gonadotropins. It is highly debated in whom and how insulin resistance should be diagnosed and treated among patients with AEDs, including PCOS. It is not suitable to administer an insulin sensitizer relying on only some mathematical models used for estimating insulin resistance. Instead, the treatment decision should be based on the constellation of the signs, symptoms and presence of obesity; acanthosis nigricans; and some laboratory abnormalities such as impaired glucose tolerance and impaired fasting glucose.
胰岛素对细胞生长、代谢和分化具有复杂的影响,这些影响由细胞表面结合受体介导,并最终引发一系列细胞内信号转导事件。在胰岛素的多种代谢和促生长作用中,胰岛素抵抗被定义为胰岛素对葡萄糖代谢的作用减弱,主要表现为血糖进入骨骼肌和脂肪组织的输出受限。另一方面,并非所有信号通路和胰岛素反应性组织都会受到同等影响,胰岛素的某些非代谢作用会过度表达。卵巢和肾上腺是对胰岛素作用仍保持敏感的组织的两个例子,胰岛素可能会导致雄激素分泌增加。多囊卵巢综合征(PCOS)是雄激素过多症(AED)最常见的形式,其发病机制与胰岛素抵抗密切相关。特发性多毛症患者也表现出胰岛素抵抗,尽管程度低于PCOS患者。虽然不像在PCOS中那么明显,但先天性肾上腺皮质增生患者可能存在胰岛素抵抗,在糖皮质激素过度治疗和肥胖的情况下,这种抵抗可能会进一步加剧。在严重胰岛素抵抗综合征患者中,无论疾病类型如何,高胰岛素血症均独立于促性腺激素促进卵巢雄激素合成。对于包括PCOS在内的AED患者,究竟谁应该被诊断为胰岛素抵抗以及如何治疗,目前存在激烈的争论。仅依靠一些用于估计胰岛素抵抗的数学模型来使用胰岛素增敏剂是不合适的。相反,治疗决策应基于体征、症状以及肥胖的存在情况;黑棘皮症;以及一些实验室异常,如糖耐量受损和空腹血糖受损。