Luo Li, Qin Zuoan, Shi Ruizheng, Ge Liangqing
Department of Cardiology, Changde First People's Hospital, Changde, China.
Department of Cardiology, Xiangya Hospital, Central South University, Changsha, China.
Front Cardiovasc Med. 2021 Apr 28;8:659821. doi: 10.3389/fcvm.2021.659821. eCollection 2021.
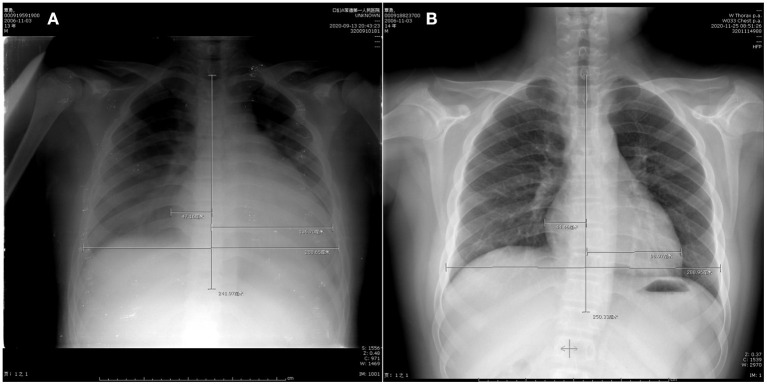
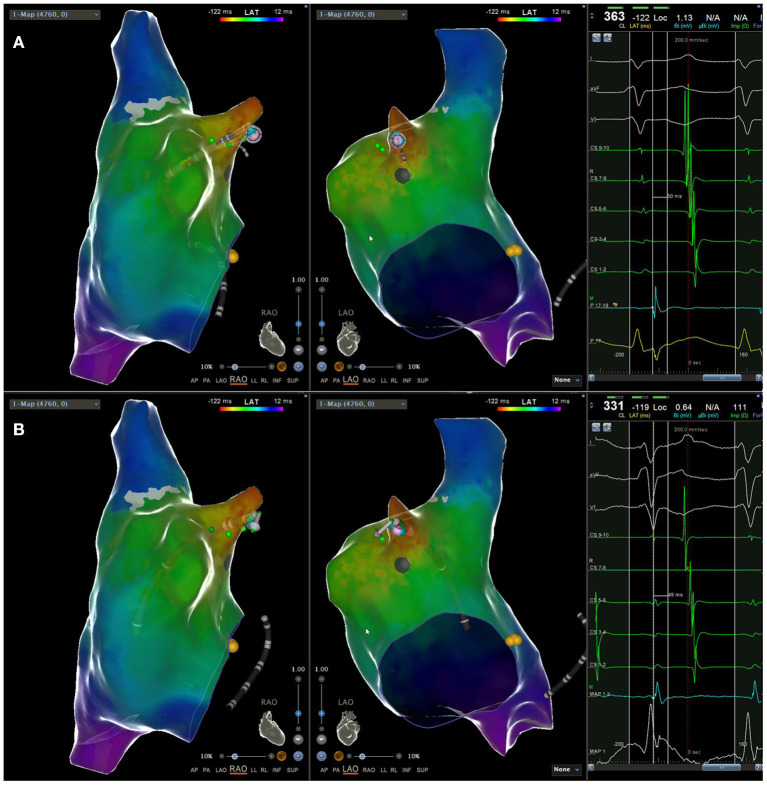
Atrial tachycardia originating from the right atrial appendage has a higher probability of failure of catheter ablation. Here we report a case of a 13-year-old boy with incessant tachycardia, complicated by heart enlargement, and heart failure. Electrophysiological examination showed that atrial tachycardia (AT) originated from the apex of the right atrial appendage, and endocardial catheter ablation was ineffective. After thoracoscopic approach, the right atrial appendage was successfully ablated with bipolar radiofrequency ablation forceps, atrial tachycardia was terminated and sinus rhythm was restored. Within 3 months since the patient was discharged from the hospital, no arrhythmia occurred and the heart structure returned to normal. Thus, thoracoscopic clamp radiofrequency ablation may be a reasonable choice for young patients with atrial tachycardia originated from the right atrial appendage when transendocardial ablation is not effective.
起源于右心耳的房性心动过速导管消融失败的概率较高。在此,我们报告一例13岁男孩,患有持续性心动过速,并发心脏扩大和心力衰竭。电生理检查显示房性心动过速(AT)起源于右心耳尖部,心内膜导管消融无效。经胸腔镜手术,使用双极射频消融钳成功消融右心耳,终止了房性心动过速并恢复窦性心律。患者出院后3个月内未发生心律失常,心脏结构恢复正常。因此,当经心内膜消融无效时,胸腔镜钳夹射频消融可能是起源于右心耳的房性心动过速年轻患者的合理选择。