McVaney Kevin E, Pepe Paul E, Maloney Lauren M, Bronsky E Stein, Crowe Remle P, Augustine James J, Gilliam Sheaffer O, Asaeda Glenn H, Eckstein Marc, Mattu Amal, Fumagalli Roberto, Aufderheide Tom P, Osterholm Michael T
Department of Emergency Medicine, University of Colorado School of Medicine, Denver, CO, USA.
Denver Health and Hospital Authority, Denver, CO, USA.
EClinicalMedicine. 2021 Apr 7;34:100815. doi: 10.1016/j.eclinm.2021.100815. eCollection 2021 Apr.
Though variable, many major metropolitan cities reported profound and unprecedented increases in out-of-hospital cardiac arrest (OHCA) in early 2020. This study examined the relative magnitude of those increases and their relationship to COVID-19 prevalence.
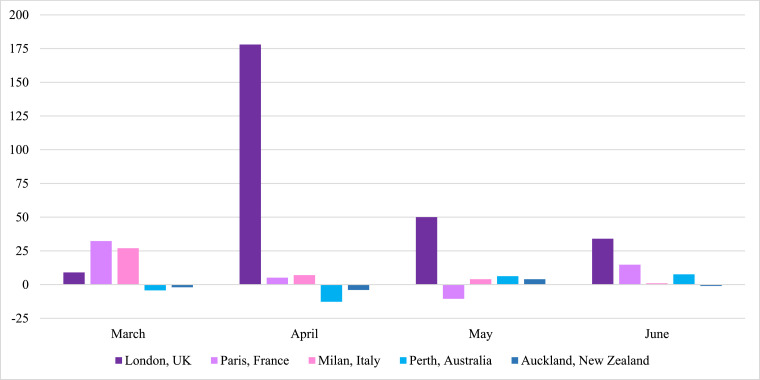
EMS (9-1-1 system) medical directors for 50 of the largest U.S. cities agreed to provide the aggregate, de-identified, pre-existing monthly tallies of OHCA among adults (age >18 years) occurring between January and June 2020 within their respective jurisdictions. Identical comparison data were also provided for corresponding time periods in 2018 and 2019. Equivalent data were obtained from the largest cities in Italy, United Kingdom and France, as well as Perth, Australia and Auckland, New Zealand.
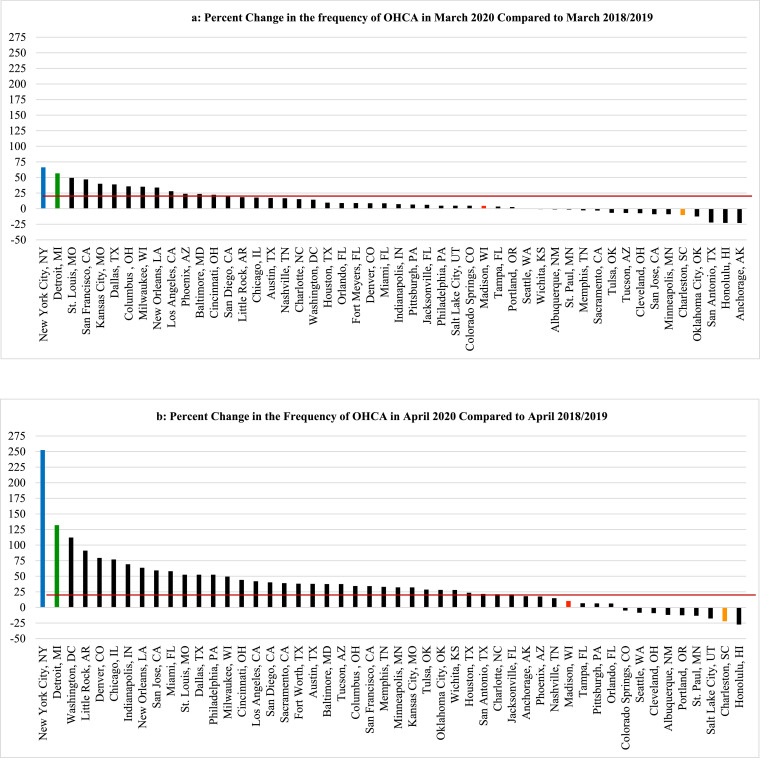
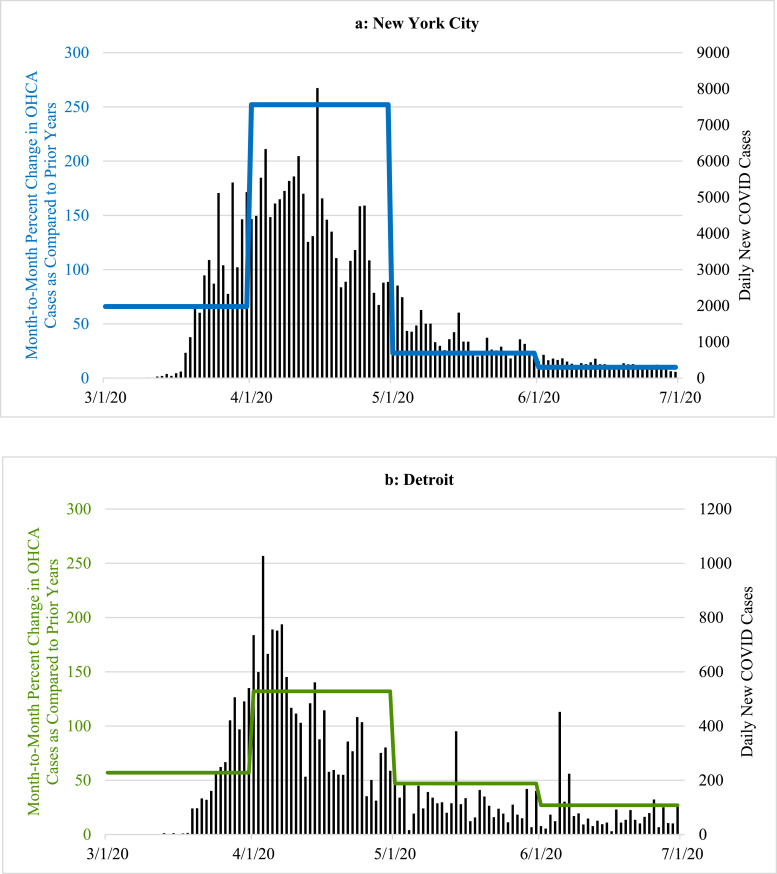
Significant OHCA escalations generally paralleled local prevalence of COVID-19. During April, most U.S. cities (34/50) had >20% increases in OHCA versus 2018-2019 which reflected high local COVID-19 prevalence. Thirteen observed 1·5-fold increases in OHCA and three COVID-19 epicenters had >100% increases (2·5-fold in New York City). Conversely, cities with lesser COVID-19 impact observed unchanged (or even diminished) OHCA numbers. Altogether ( = 50), on average, OHCA cases/city rose 59% during April ( = 0·03). By June, however, after mitigating COVID-19 spread, cities with the highest OHCA escalations returned to (or approached) pre-COVID OHCA numbers while cities minimally affected by COVID-19 during April (and not experiencing OHCA increases), then had marked OHCA escalations when COVID-19 began to surge locally. European, Australian, and New Zealand cities mirrored the U.S. experience.
Most metropolitan cities experienced profound escalations of OHCA generally paralleling local prevalence of COVID-19. Most of these patients were pronounced dead without COVID-19 testing.
No funding was involved. Cities provided de-identified aggregate data collected routinely for standard quality assurance functions.
尽管情况各异,但许多主要大城市报告称,2020年初院外心脏骤停(OHCA)出现了深刻且前所未有的增加。本研究调查了这些增加的相对幅度及其与新冠病毒(COVID-19)流行率的关系。
美国50个最大城市的紧急医疗服务(911系统)医疗主任同意提供2020年1月至6月期间其各自辖区内18岁以上成年人OHCA的汇总、匿名、既往月度统计数据。还提供了2018年和2019年相应时间段的相同比较数据。从意大利、英国和法国的最大城市以及澳大利亚的珀斯和新西兰的奥克兰获取了等效数据。
OHCA的显著增加通常与当地COVID-19的流行情况平行。在4月份,大多数美国城市(34/50)的OHCA较2018 - 2019年增加了20%以上,这反映了当地COVID-19的高流行率。13个城市观察到OHCA增加了1.5倍,3个COVID-19疫情中心增加了100%以上(纽约市为2.5倍)。相反,受COVID-19影响较小的城市OHCA数量保持不变(甚至减少)。总体而言(n = 50),4月份每个城市的OHCA病例平均增加了59%(p = 0.03)。然而,到6月份,在缓解了COVID-19的传播后,OHCA增加幅度最大的城市恢复到(或接近)COVID-19之前的OHCA数量,而4月份受COVID-19影响最小(且OHCA没有增加)的城市,在当地COVID-19开始激增时OHCA出现了显著增加。欧洲、澳大利亚和新西兰的城市情况与美国类似。
大多数大城市的OHCA出现了显著增加,总体上与当地COVID-19的流行情况平行。这些患者中的大多数在未进行COVID-19检测的情况下被宣布死亡。
本研究未涉及资金。各城市提供了为标准质量保证功能而常规收集的匿名汇总数据。