Yang Dan-Hong, Wang Wei-Ping, Zhang Qiang, Pan Hong-Ying, Huang Yi-Cheng, Zhang Jia-Jie
Department of Infectious Diseases, Zhejiang Provincial People's Hospital, People's Hospital of Hangzhou Medical College, Hangzhou 310014, Zhejiang Province, China.
Postgraduate Department, Bengbu Medical College, Bengbu 233030, Anhui Province, China.
World J Gastroenterol. 2021 May 7;27(17):2025-2038. doi: 10.3748/wjg.v27.i17.2025.
Antiviral therapy cannot completely block the progression of hepatitis B to hepatocellular carcinoma (HCC). Furthermore, there are few predictors of early HCC progression and limited strategies to prevent progression in patients with HBV-related cirrhosis who receive nucleos(t)ide analog (NA) therapy.
The study aim was to clarify risk factors and the diagnostic value of alpha-fetoprotein (AFP) for HCC progression in NA-treated hepatitis B virus (HBV)-related cirrhosis patients.
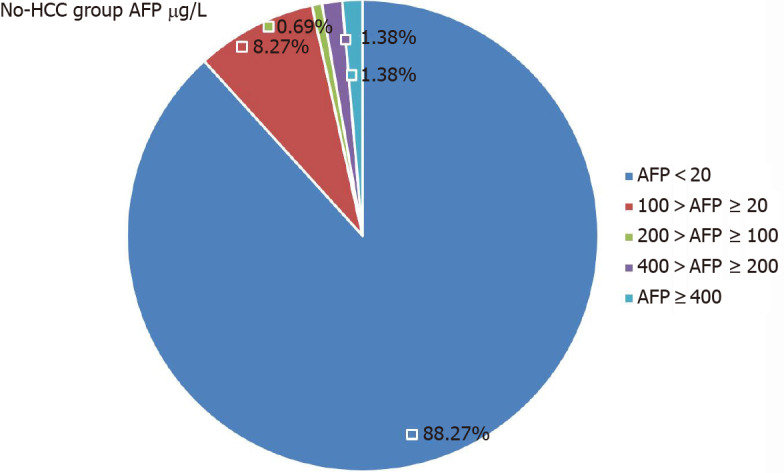
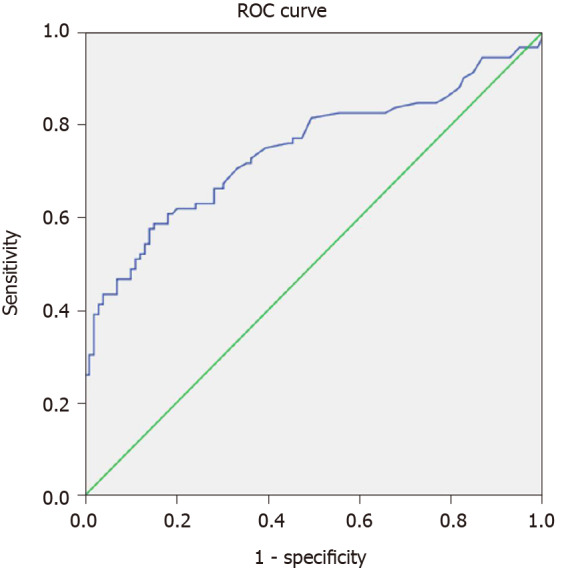
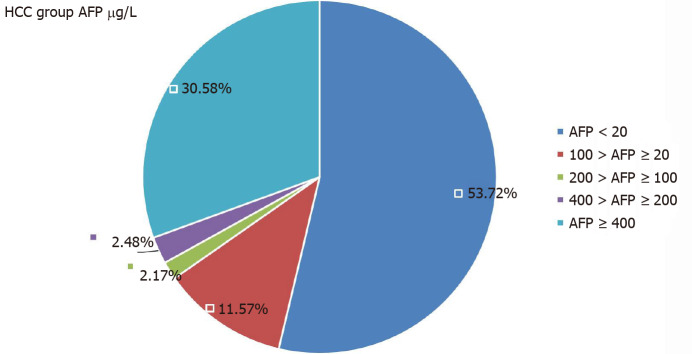
In this retrospective cross-sectional study, we analyzed the clinical data of 266 patients with HBV-related cirrhosis who received NA treatment between February 2014 and April 2020 at Zhejiang Provincial People's Hospital. The patients were divided into two groups, 145 who did not progress to HCC (No-HCC group), and 121 who progressed to HCC during NA treatment (HCC group). The logistic regression analysis was used to analyze the risk factors of HCC progression. The diagnostic value of AFP for HCC was evaluated by receiver operating characteristic (ROC) curve analysis.
Univariate analysis showed that age ≥ 60 years ( = 0.001), hepatitis B and alcoholic etiology ( = 0.007), smoking history ( < 0.001), family history of HBV-related HCC ( = 0.002), lamivudine resistance ( = 0.011), HBV DNA negative ( = 0.023), aspartate aminotransferase > 80 U/L ( = 0.002), gamma-glutamyl transpeptidase > 120 U/L ( = 0.001), alkaline phosphatase > 250 U/L ( = 0.001), fasting blood glucose (FBG) ≥ 6.16 (mmol/L) ( = 0.001) and Child-Pugh class C ( = 0.005) were correlated with HCC progression. In multivariate analysis, age ≥ 60 years [hazard ratio (HR) = 3.089, 95% confidence interval (CI): 1.437-6.631, = 0.004], smoking history (HR = 4.001, 95%CI: 1.836-8.716, < 0.01), family history of HBV-related HCC (HR = 6.763, 95%CI: 1.253-36.499, < 0.05), lamivudine resistance (HR = 2.949, 95%CI: 1.207-7.208, = 0.018), HBV DNA negative (HR = 0.026, 95%CI: 0.007-0.139, < 0.01), FBG ≥ 6.16 mmol/L (HR = 7.219, 95%CI: 3.716-14.024, < 0.01) were independent risk factors of HCC progression. ROC of AFP for diagnosis of HCC was 0.746 (95%CI: 0.674-0.818). A cutoff value of AFP of 9.00 ug/L had a sensitivity of 0.609, and specificity of 0.818 for diagnosing HCC.
Age ≥ 60 years, smoking history, family history of HCC, lamivudine resistance, HBV DNA negative, FBG ≥ 6.16 mmol/L were risk factors of HCC progression. Serum AFP had limited diagnostic value for HCC.
抗病毒治疗无法完全阻断乙型肝炎向肝细胞癌(HCC)的进展。此外,对于接受核苷(酸)类似物(NA)治疗的HBV相关肝硬化患者,早期HCC进展的预测指标很少,预防进展的策略也有限。
本研究旨在阐明NA治疗的乙型肝炎病毒(HBV)相关肝硬化患者中HCC进展的危险因素及甲胎蛋白(AFP)的诊断价值。
在这项回顾性横断面研究中,我们分析了2014年2月至2020年4月期间在浙江省人民医院接受NA治疗的266例HBV相关肝硬化患者的临床资料。患者分为两组,145例未进展为HCC的患者(非HCC组),以及121例在NA治疗期间进展为HCC的患者(HCC组)。采用逻辑回归分析来分析HCC进展的危险因素。通过受试者工作特征(ROC)曲线分析评估AFP对HCC的诊断价值。
单因素分析显示,年龄≥60岁(P = 0.001)、乙型肝炎合并酒精性病因(P = 0.007)、吸烟史(P < 0.001)、HBV相关HCC家族史(P = 0.002)、拉米夫定耐药(P = 0.011)、HBV DNA阴性(P = 0.023)、天冬氨酸氨基转移酶> 80 U/L(P = 0.0)、γ-谷氨酰转肽酶> 120 U/L(P = 0.001)、碱性磷酸酶> 250 U/L(P = 0.001)、空腹血糖(FBG)≥6.16(mmol/L)(P = 0.001)以及Child-Pugh C级(P = 0.005)与HCC进展相关。多因素分析中,年龄≥60岁[风险比(HR)= 3.089,95%置信区间(CI):1.437 - 6.631,P = 0.004]、吸烟史(HR = 4.001,95%CI:1.836 - 8.716,P < 0.01)、HBV相关HCC家族史(HR = 6.763,95%CI:1.253 - 36.499,P < 0.05)、拉米夫定耐药(HR = 2.949,95%CI:1.207 - 7.208,P = 0.018)、HBV DNA阴性(HR = 0.026,95%CI:0.007 - 0.139,P < 0.01)、FBG≥6.16 mmol/L(HR = 7.219,95%CI:3.716 - 14.024,P < 0.01)是HCC进展的独立危险因素。AFP诊断HCC的ROC为0.746(95%CI:0.674 - 0.818)。AFP临界值为9.00 μg/L时,诊断HCC的灵敏度为0.609,特异度为0.818。
年龄≥60岁、吸烟史、HCC家族史、拉米夫定耐药、HBV DNA阴性、FBG≥6.16 mmol/L是HCC进展的危险因素。血清AFP对HCC的诊断价值有限。