Department of Surgical and Perioperative Sciences, Surgery, Umeå University, SE-901 85, Umeå, Sweden.
Department of Surgery, Södertälje Hospital, Södertälje, Sweden.
Langenbecks Arch Surg. 2021 Sep;406(6):1971-1977. doi: 10.1007/s00423-021-02182-0. Epub 2021 May 18.
Anterior resection is the procedure of choice for tumours in the mid and upper rectum. Depending on tumour height, a total mesorectal excision (TME) or partial mesorectal excision (PME) can be performed. Low anastomoses in particular have a high risk of developing anastomotic leakage, which might be explained by blood perfusion compromise. A pilot study indicated a worse blood flow in TME patients in an open setting. The aim of this study was to further evaluate perianastomotic blood perfusion changes in relation to TME and PME in a predominantly laparoscopic context.
In this prospective cohort study, laser Doppler flowmetry was used to evaluate the perianastomotic colonic and rectal perfusion before and after surgery. The two surgical techniques were compared in terms of mean differences of perfusion units using a repeated measures ANOVA design, which also enabled interaction analyses between type of mesorectal excision and location of measurement. Anastomotic leakage until 90 days after surgery was reported for descriptive purposes.
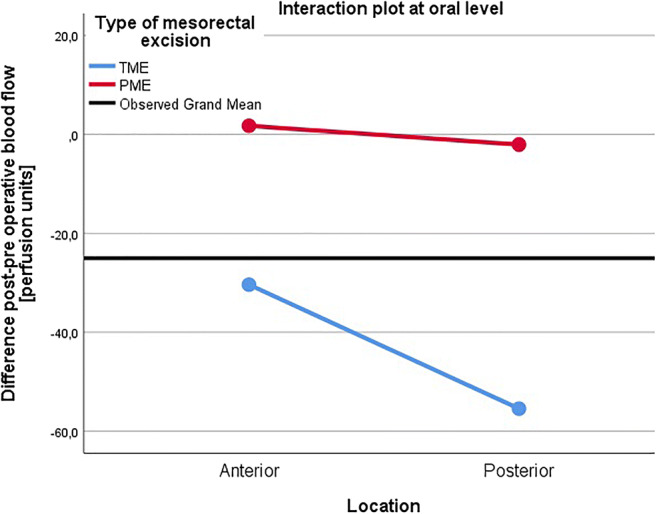
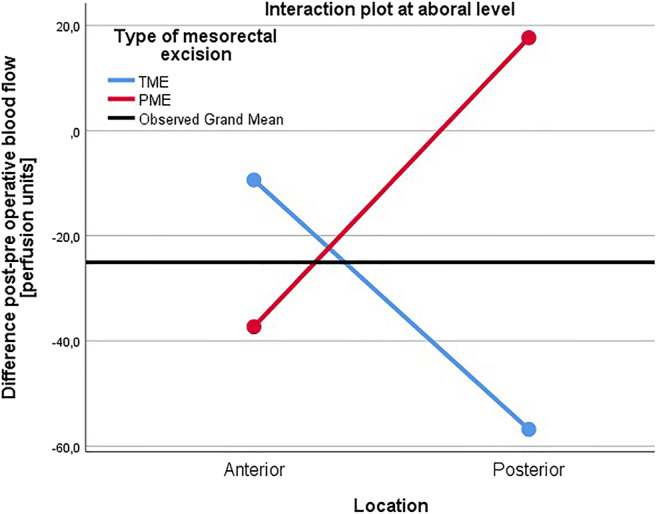
Some 28 patients were available for analysis: 17 TME and 11 PME patients. TME patients had a reduced blood perfusion postoperatively compared to PME patients in the aboral posterior area (mean difference: -57 vs 18 perfusion units; p = 0.010). An interaction between mesorectal excision type and anterior/posterior location was detected at the aboral level (p = 0.007). Two patients developed a minor leakage, diagnosed after discharge.
Patients operated on using TME have a decreased blood flow in the aboral posterior quadrant of the rectum postoperatively compared to patients operated on using PME. This might explain differing rates of anastomotic leakage.
ClinicalTrials.gov Identifier: NCT02401100.
前切除术是治疗中高位直肠肿瘤的首选方法。根据肿瘤的高度,可以进行全直肠系膜切除术(TME)或部分直肠系膜切除术(PME)。低位吻合尤其有发生吻合口漏的高风险,这可能与血液灌注受损有关。一项初步研究表明,在开放环境下,TME 患者的血流情况更差。本研究旨在进一步评估在以腹腔镜为主的环境下,TME 和 PME 与吻合口周围血液灌注变化的关系。
在这项前瞻性队列研究中,激光多普勒流量仪用于评估手术前后吻合口周围结肠和直肠的灌注情况。使用重复测量方差分析设计比较两种手术技术的灌注单位平均值差异,该设计还可以进行 TME 和 PME 之间的交互分析以及测量位置之间的交互分析。描述性地报告手术后 90 天内的吻合口漏。
28 例患者可用于分析:17 例 TME 患者和 11 例 PME 患者。与 PME 患者相比,TME 患者的吻合口后远段后区的血流灌注减少(平均差异:-57 与 18 个灌注单位;p = 0.010)。在远段水平检测到 TME 类型和前/后位置之间的交互作用(p = 0.007)。有 2 例患者在出院后诊断出轻度漏液。
与接受 PME 手术的患者相比,接受 TME 手术的患者术后直肠远段后区的血流减少。这可能解释了不同的吻合口漏发生率。
ClinicalTrials.gov 标识符:NCT02401100。