Henry Ford Cancer Institute, Henry Ford Health System, Detroit, Michigan, USA.
Syapse, San Francisco, California, USA.
Cancer Rep (Hoboken). 2021 Oct;4(5):e1388. doi: 10.1002/cnr2.1388. Epub 2021 May 20.
The understanding of the impact of COVID-19 in patients with cancer is evolving, with need for rapid analysis.
This study aims to compare the clinical and demographic characteristics of patients with cancer (with and without COVID-19) and characterize the clinical outcomes of patients with COVID-19 and cancer.
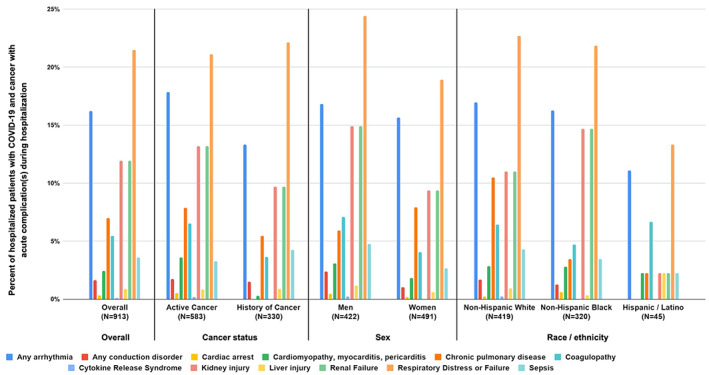
Real-world data (RWD) from two health systems were used to identify 146 702 adults diagnosed with cancer between 2015 and 2020; 1267 COVID-19 cases were identified between February 1 and July 30, 2020. Demographic, clinical, and socioeconomic characteristics were extracted. Incidence of all-cause mortality, hospitalizations, and invasive respiratory support was assessed between February 1 and August 14, 2020. Among patients with cancer, patients with COVID-19 were more likely to be Non-Hispanic black (NHB), have active cancer, have comorbidities, and/or live in zip codes with median household income <$30 000. Patients with COVID-19 living in lower-income areas and NHB patients were at greatest risk for hospitalization from pneumonia, fluid and electrolyte disorders, cough, respiratory failure, and acute renal failure and were more likely to receive hydroxychloroquine. All-cause mortality, hospital admission, and invasive respiratory support were more frequent among patients with cancer and COVID-19. Male sex, increasing age, living in zip codes with median household income <$30 000, history of pulmonary circulation disorders, and recent treatment with immune checkpoint inhibitors or chemotherapy were associated with greater odds of all-cause mortality in multivariable logistic regression models.
RWD can be rapidly leveraged to understand urgent healthcare challenges. Patients with cancer are more vulnerable to COVID-19 effects, especially in the setting of active cancer and comorbidities, with additional risk observed in NHB patients and those living in zip codes with median household income <$30 000.
对癌症患者中 COVID-19 影响的认识在不断发展,需要快速分析。
本研究旨在比较患有癌症(有 COVID-19 和无 COVID-19)的患者的临床和人口统计学特征,并描述 COVID-19 合并癌症患者的临床结局。
利用两个医疗系统的真实世界数据(RWD),在 2015 年至 2020 年间,识别出 146702 名患有癌症的成年人;在 2020 年 2 月 1 日至 7 月 30 日期间,确定了 1267 例 COVID-19 病例。提取了人口统计学、临床和社会经济特征。在 2020 年 2 月 1 日至 8 月 14 日期间,评估了所有原因死亡率、住院率和有创性呼吸支持的发生率。在患有癌症的患者中,患有 COVID-19 的患者更有可能是非西班牙裔黑人(NHB),患有活动性癌症,合并症较多,或居住在中位家庭收入<30000 美元的邮政编码地区。来自肺炎、液体和电解质紊乱、咳嗽、呼吸衰竭和急性肾衰竭的住院风险最高的是住在低收入地区的 COVID-19 患者和 NHB 患者,并且更有可能接受羟氯喹治疗。患有 COVID-19 和癌症的患者的全因死亡率、住院率和有创性呼吸支持率均较高。多变量逻辑回归模型显示,男性、年龄增长、居住在中位家庭收入<30000 美元的邮政编码地区、有肺循环障碍病史以及最近接受免疫检查点抑制剂或化疗治疗与全因死亡率的几率增加相关。
RWD 可快速用于了解紧急医疗保健挑战。癌症患者更容易受到 COVID-19 影响,特别是在患有活动性癌症和合并症的情况下,NHB 患者和中位家庭收入<30000 美元的邮政编码地区的患者存在额外风险。