KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya.
Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK.
Malar J. 2021 May 20;20(1):227. doi: 10.1186/s12936-021-03758-3.
The over-distributed pattern of malaria transmission has led to attempts to define malaria "hotspots" that could be targeted for purposes of malaria control in Africa. However, few studies have investigated the use of routine health facility data in the more stable, endemic areas of Africa as a low-cost strategy to identify hotspots. Here the objective was to explore the spatial and temporal dynamics of fever positive rapid diagnostic test (RDT) malaria cases routinely collected along the Kenyan Coast.
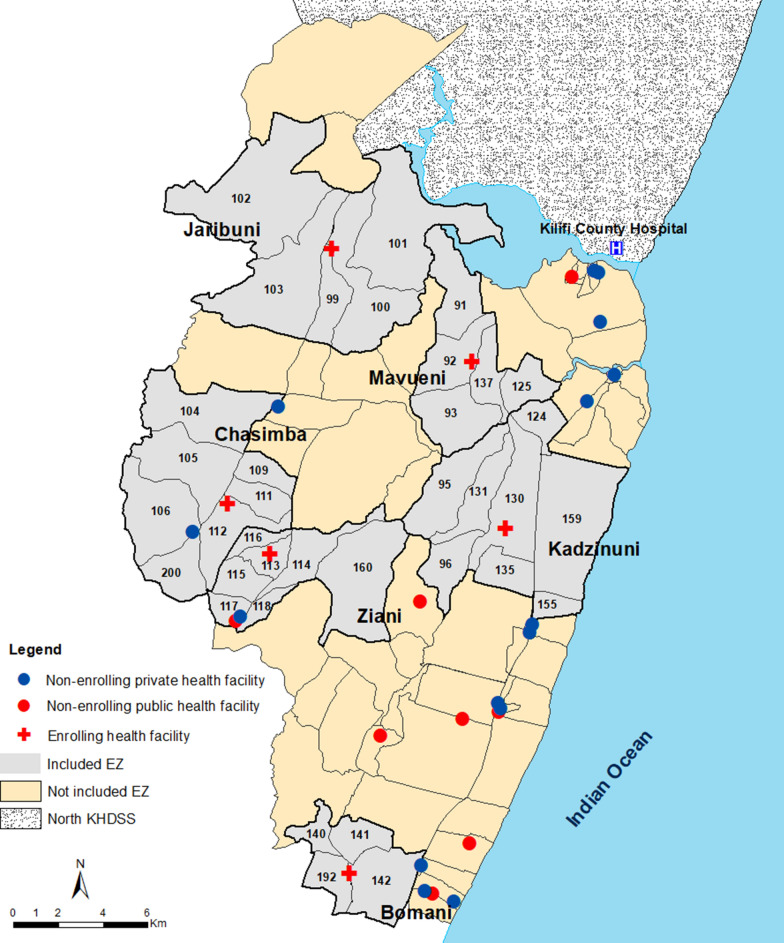
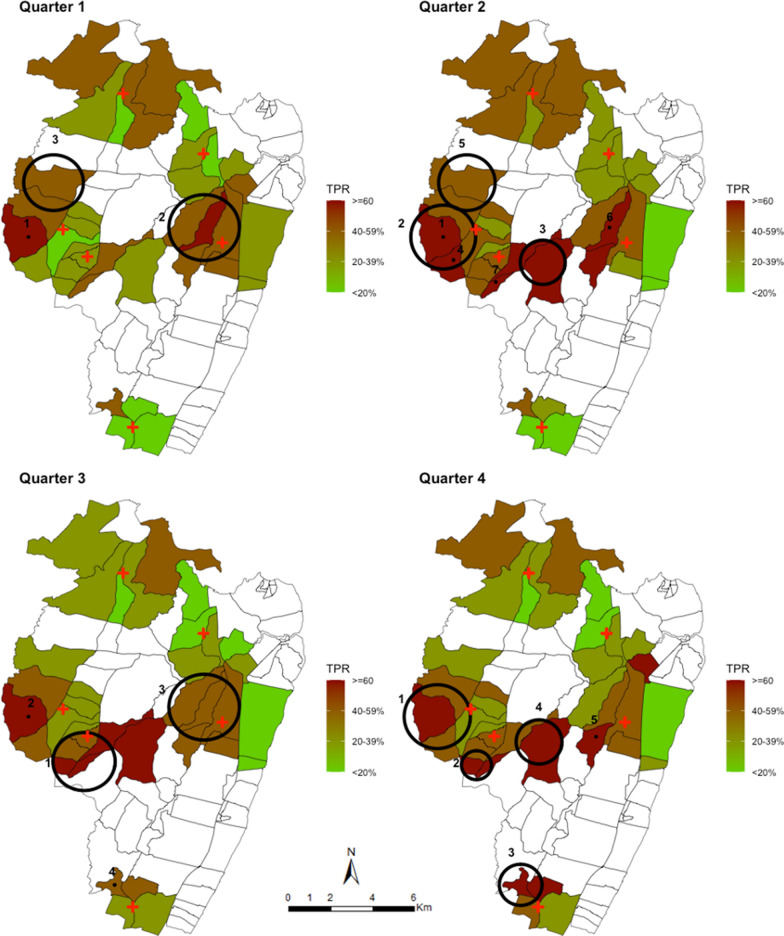
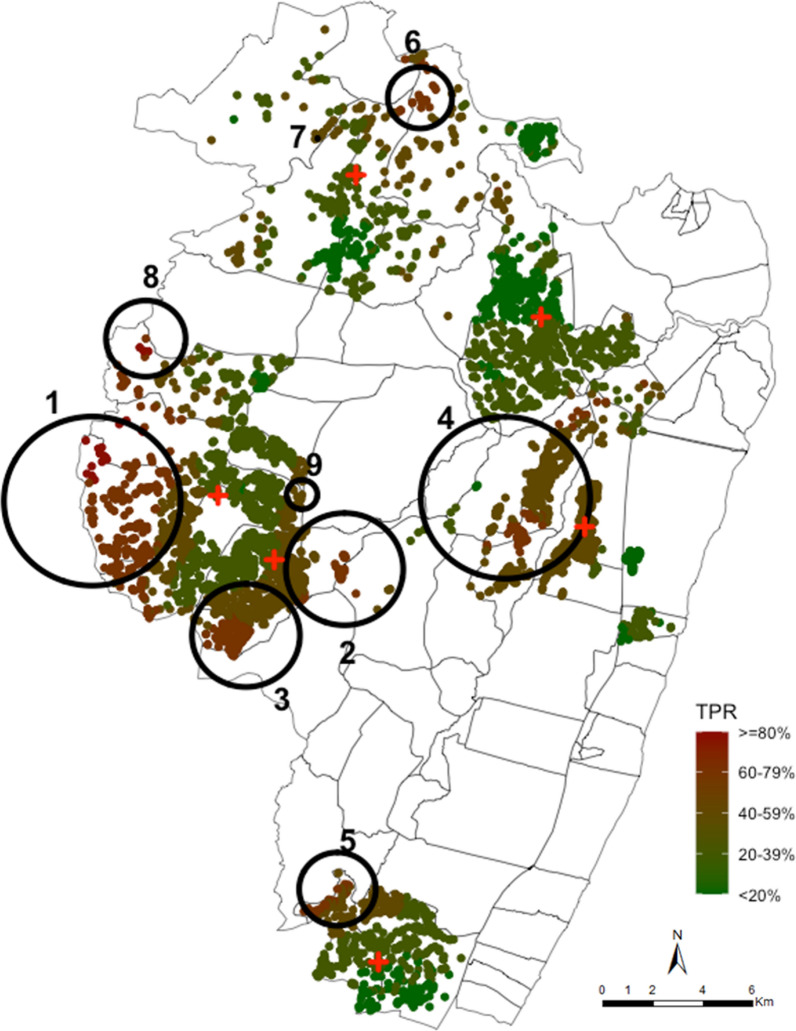
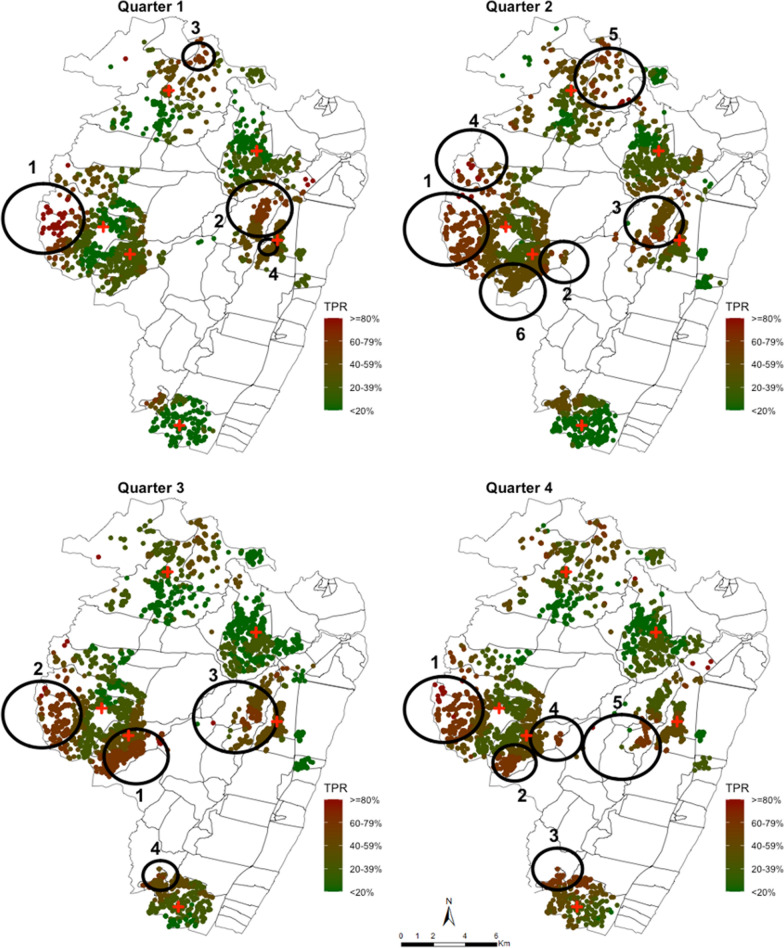
Data on fever positive RDT cases between March 2018 and February 2019 were obtained from patients presenting to six out-patients health-facilities in a rural area of Kilifi County on the Kenyan Coast. To quantify spatial clustering, homestead level geocoded addresses were used as well as aggregated homesteads level data at enumeration zone. Data were sub-divided into quarterly intervals. Kulldorff's spatial scan statistics using Bernoulli probability model was used to detect hotspots of fever positive RDTs across all ages, where cases were febrile individuals with a positive test and controls were individuals with a negative test.
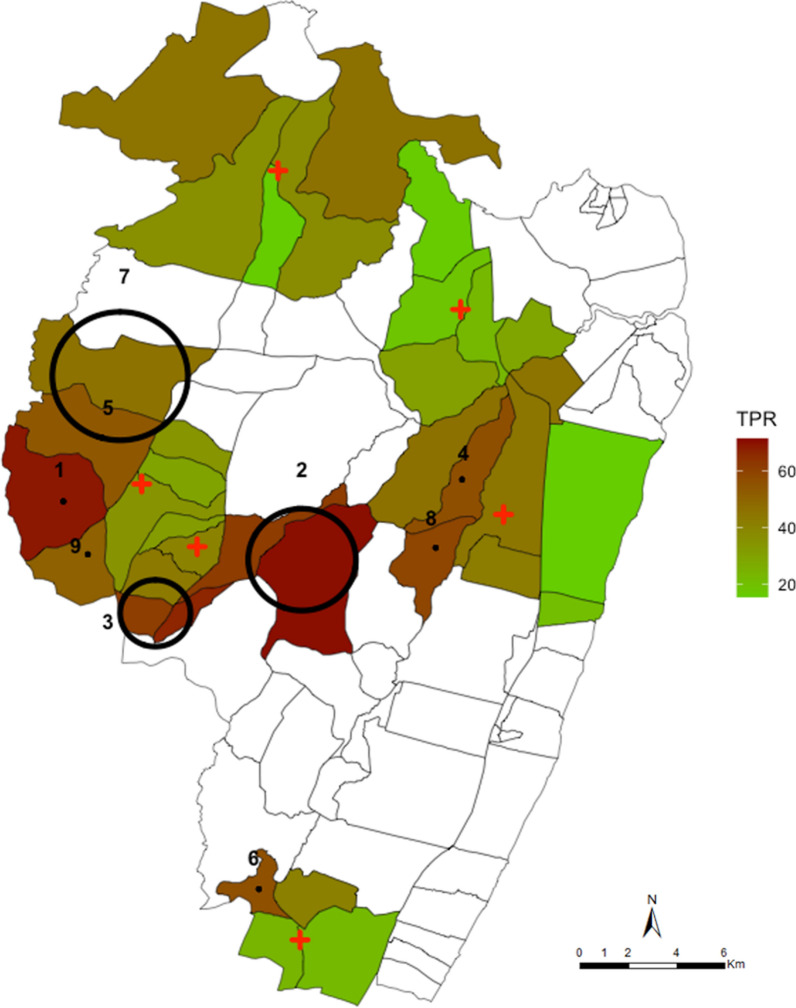
Across 12 months of surveillance, there were nine significant clusters that were identified using the spatial scan statistics among RDT positive fevers. These clusters included 52% of all fever positive RDT cases detected in 29% of the geocoded homesteads in the study area. When the resolution of the data was aggregated at enumeration zone (village) level the hotspots identified were located in the same areas. Only two of the nine hotspots were temporally stable accounting for 2.7% of the homesteads and included 10.8% of all fever positive RDT cases detected.
Taking together the temporal instability of spatial hotspots and the relatively modest fraction of the malaria cases that they account for; it would seem inadvisable to re-design the sub-county control strategies around targeting hotspots.
疟疾传播的过度分布模式导致人们试图定义疟疾“热点”,以便在非洲进行疟疾控制。然而,很少有研究调查在非洲更稳定的地方性地区使用常规卫生机构数据作为一种低成本策略来识别热点。在这里,目的是探索在肯尼亚沿海地区常规收集的发热阳性快速诊断检测(RDT)疟疾病例的时空动态。
从肯尼亚沿海基利菲县一个农村地区的六家门诊卫生机构就诊的发热患者中获得了 2018 年 3 月至 2019 年 2 月间发热阳性 RDT 病例的数据。为了量化空间聚类,使用了家庭级别的地理编码地址以及聚集的家庭级别数据在计数区。数据分为四个季度。使用伯努利概率模型的 Kulldorff 空间扫描统计数据来检测所有年龄段发热阳性 RDT 的热点,其中病例是发热且检测阳性的个体,对照是检测阴性的个体。
在 12 个月的监测中,使用空间扫描统计数据在 RDT 阳性发热中发现了九个显著的聚类。这些聚类包括研究区域 29%的地理编码家庭中检测到的所有发热阳性 RDT 病例的 52%。当数据的分辨率在计数区(村庄)级别聚集时,确定的热点位于相同的区域。在九个热点中,只有两个具有时间稳定性,占家庭的 2.7%,包括检测到的所有发热阳性 RDT 病例的 10.8%。
考虑到时空热点的不稳定性以及它们所代表的疟疾病例相对较少;似乎不建议围绕目标热点重新设计次县控制策略。