Ahmanson Translational Theranostics Division, Department of Molecular & Medical Pharmacology, University of California Los Angeles, Los Angeles, California.
Department of Nuclear Medicine, Technical University Munich, Klinikum rechts der Isar, Munich, Germany.
J Nucl Med. 2021 Oct;62(10):1440-1446. doi: 10.2967/jnumed.121.261982. Epub 2021 May 20.
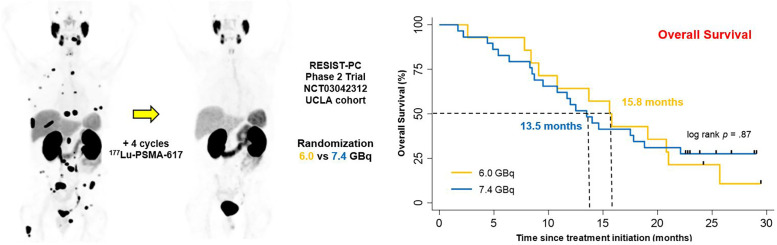
The objective of this study was to determine prospectively the efficacy profile of 2 activity regimens of Lu-PSMA therapy in patients with progressive metastatic castrate-resistant prostate cancer (mCRPC): 6.0 vs. 7.4 GBq. RESIST-PC (NCT03042312) was a prospective multicenter phase 2 trial. Patients with progressive mCRPC after ≥ 1 novel androgen-axis drug, either chemotherapy naïve or postchemotherapy, with sufficient bone marrow reserve, normal kidney function, and sufficient PSMA expression by PSMA PET were eligible. Patients were randomized (1:1) into 2 activity groups (6.0 or 7.4 GBq) and received up to 4 cycles every 8 wk. The primary endpoint was the efficacy of Lu-PSMA measured by the prostate-specific antigen (PSA) response rate (RR) after 2 cycles (≥50% decline from baseline). Secondary endpoints included the PSA RR (≥50% decline) at any time (best response), and overall survival (OS). The study was closed at enrollment of 71/200 planned patients because of sponsorship transfer. We report here the efficacy of the University of California Los Angeles cohort results only ( = 43). The PSA RRs after 2 cycles and at any time were 11/40 (28%, 95% CI 15-44), 6/13 (46%, 95% CI 19-75), and 5/27 (19%, 95% CI 6-38), and 16/43 (37%, 95% CI 23-53), 7/14 (50%, 95% CI 23-77), and 9/29 (31%, 95% CI 15-51) in the whole cohort, the 6.0-GBq group, and the 7.4-GBq group, respectively ( = 0.12 and = 0.31). The median OS was 14.0 mo (95% CI 10.1-17.9), 15.8 (95% CI 11.8-19.4), and 13.5 (95% CI 10.0-17.0) in the whole cohort, the 6.0-GBq group, and the 7.4 GBq group, respectively ( = 0.87). OS was longer in patients who experienced a PSA decline ≥ 50% at any time than in those who did not: median, 20.8 versus 10.8 mo ( = 0.005). In this prospective phase 2 trial of Lu-PSMA for mCRPC, the median OS was 14 mo. Despite the heterogeneous study population and the premature study termination, the efficacy profile of Lu-PSMA appeared to be favorable and comparable with both activity regimens (6.0 vs. 7.4 GBq). Results justify confirmation with real-world data matched-pair analysis and further clinical trials to refine and optimize the Lu-PSMA therapy administration scheme to improve tumor radiation dose delivery and efficacy.
这项研究的目的是前瞻性地确定两种 Lu-PSMA 治疗方案在进展性转移性去势抵抗性前列腺癌(mCRPC)患者中的疗效特征:6.0 与 7.4GBq。RESIST-PC(NCT03042312)是一项前瞻性多中心 2 期试验。符合条件的患者为:在接受≥1 种新型雄激素轴药物治疗后出现进展性 mCRPC,无论是否接受过化疗,骨髓储备充足,肾功能正常,PSMA 表达通过 PSMA PET 充分表达。患者按 1:1 随机分配至 2 个活性组(6.0 或 7.4GBq),每 8 周接受最多 4 个周期的治疗。主要终点是 Lu-PSMA 的疗效,通过前列腺特异性抗原(PSA)应答率(RR)来衡量,即与基线相比下降≥50%。次要终点包括任何时间(最佳反应)的 PSA RR(≥50%下降)和总生存期(OS)。由于赞助转移,该研究在计划入组的 200 名患者中的 71 名入组后关闭。我们仅在此报告加利福尼亚大学洛杉矶分校队列结果的疗效( = 43)。2 个周期和任何时间的 PSA RR 分别为 11/40(28%,95%CI 15-44)、6/13(46%,95%CI 19-75)和 5/27(19%,95%CI 6-38),16/43(37%,95%CI 23-53)、7/14(50%,95%CI 23-77)和 9/29(31%,95%CI 15-51),在整个队列、6.0-Gbq 组和 7.4-Gbq 组中( = 0.12 和 = 0.31)。整个队列、6.0-Gbq 组和 7.4-Gbq 组的中位 OS 分别为 14.0mo(95%CI 10.1-17.9)、15.8mo(95%CI 11.8-19.4)和 13.5mo(95%CI 10.0-17.0)( = 0.87)。在任何时间 PSA 下降≥50%的患者中,OS 较长:中位 OS 为 20.8 个月,而 PSA 无下降患者的中位 OS 为 10.8 个月( = 0.005)。在这项针对 mCRPC 的 Lu-PSMA 的前瞻性 2 期试验中,中位 OS 为 14 个月。尽管研究人群存在异质性且研究提前终止,但 Lu-PSMA 的疗效特征似乎是有利的,与两种活性方案(6.0 与 7.4GBq)相当。结果证明,使用真实世界数据匹配对分析和进一步的临床试验进行证实是合理的,这将有助于优化 Lu-PSMA 治疗方案,以提高肿瘤辐射剂量输送和疗效。