Hospital Clínic, IDIBAPS, University of Barcelona, Barcelona, Spain.
Royal Adelaide Hospital and Flinders Medical Centre, Adelaide, SA, Australia.
Leukemia. 2021 Dec;35(12):3455-3465. doi: 10.1038/s41375-021-01261-x. Epub 2021 May 20.
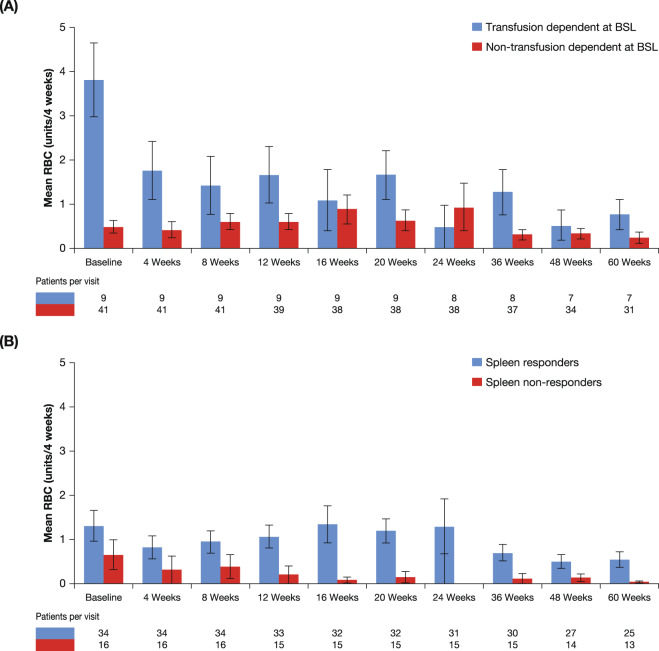
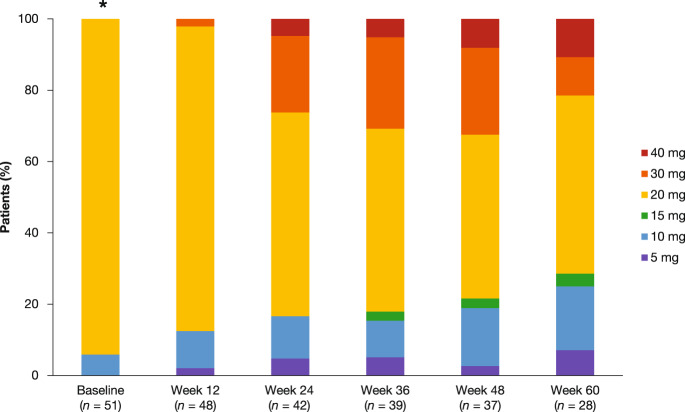
Anemia is a frequent manifestation of myelofibrosis (MF) and there is an unmet need for effective treatments in anemic MF patients. The REALISE phase 2 study (NCT02966353) evaluated the efficacy and safety of a novel ruxolitinib dosing strategy with a reduced starting dose with delayed up-titration in anemic MF patients. Fifty-one patients with primary MF (66.7%), post-essential thrombocythemia MF (21.6%), or post-polycythemia vera MF (11.8%) with palpable splenomegaly and hemoglobin <10 g/dl were included. Median age was 67 (45-88) years, 41.2% were female, and 18% were transfusion-dependent. Patients received 10 mg ruxolitinib b.i.d. for the first 12 weeks, then up-titrations of up to 25 mg b.i.d. were permitted, based on efficacy and platelet counts. Overall, 70% of patients achieved a ≥50% reduction in palpable spleen length at any time during the study. The most frequent adverse events leading to dose interruption/adjustment were thrombocytopenia (17.6%) and anemia (11.8%). Patients who had a dose increase had greater spleen size and higher white blood cell counts at baseline. Median hemoglobin levels remained stable and transfusion requirements did not increase compared with baseline. These results reinforce the notion that it is unnecessary to delay or withhold ruxolitinib because of co-existent or treatment-emergent anemia.
贫血是骨髓纤维化(MF)的常见表现,对于贫血性 MF 患者,存在未满足的有效治疗需求。REALISE 期 2 研究(NCT02966353)评估了一种新型鲁索利替尼给药策略的疗效和安全性,该策略采用较低起始剂量并延迟剂量递增,适用于贫血性 MF 患者。该研究纳入了 51 例原发性 MF(66.7%)、原发性血小板增多症后 MF(21.6%)或原发性红细胞增多症后 MF(11.8%)患者,这些患者均有可触及的脾肿大和血红蛋白<10g/dl。中位年龄为 67(45-88)岁,41.2%为女性,18%依赖输血。患者接受 10mg 鲁索利替尼每日 2 次治疗 12 周,然后根据疗效和血小板计数允许增加剂量至每日 2 次 25mg。总体而言,70%的患者在研究期间的任何时间都实现了可触及脾长度至少减少 50%。导致剂量中断/调整的最常见不良事件是血小板减少症(17.6%)和贫血(11.8%)。基线时剂量增加的患者脾肿大程度更大,白细胞计数更高。与基线相比,中位血红蛋白水平保持稳定,且输血需求未增加。这些结果进一步证实,没有必要因为并存或治疗中出现的贫血而延迟或避免使用鲁索利替尼。