From the Queen Square MS Centre (O.A.A., W.B., O.C., C.H., Y.H.), UCL Queen Square Institute of Neurology, Faculty of Brain Sciences, University College London; Department of Neurology (O.A.A., O.C., C.H., Y.H.), Great Ormond Street Hospital for Children, London; Children's Neurosciences (C.M.), Evelina London Children's Hospital, Guy's and St Thomas' NHS Foundation; Department of Paediatric Neurology (T.R., M.C.), Addenbrooke's Hospital, Cambridge; Department of Neurology (J.-C.S., R.K.), Alder Hey Children's NHS Foundation Trust, Liverpool, United Kingdom; Queen Square Institute of Neurology (C.T.), Faculty of Brain Sciences, University College London; Multiple Sclerosis Centre of Catalonia (Cemcat) (C.T.), Vall d'Hebron Institute of Research, Vall d'Hebron Barcelona Hospital Campus, Spain; Children's Neurosciences (S.B.), Evelina London Children's Hospital, Guy's and St Thomas' NHS Foundation Trust, King's Health Partners Academic Health Science Centre, London; Department of Clinical Neurosciences (A.C.), Addenbrooke's Hospital, Cambridge; Translational and Clinical Research Institute (R.F.), Newcastle University; Department of Neuroradiology (K.M.), Great Ormond Street Hospital for Children, London; Department of Neurology (D.R., S. West), Royal Manchester Children's Hospital, Manchester; Department of Neurology (S. Wright, E.W.), Birmingham Children's Hospital, Birmingham; Aston Neuroscience Institute (S. Wright, E.W.), College of Health and Life Sciences, Aston University, Birmingham, United Kingdom; Evelina London Children's Hospital (M.L.), Guy's and St Thomas' NHS Foundation Trust, King's Health Partners Academic Health Science Centre, London, United Kingdom; and NIHR University College London Hospitals Biomedical Research Centre (O.C.).
Neurol Neuroimmunol Neuroinflamm. 2021 May 21;8(4). doi: 10.1212/NXI.0000000000001008. Print 2021 Jul.
To compare the real-world effectiveness of newer disease-modifying therapies (DMTs) vs injectables in children with relapsing-remitting multiple sclerosis (RRMS).
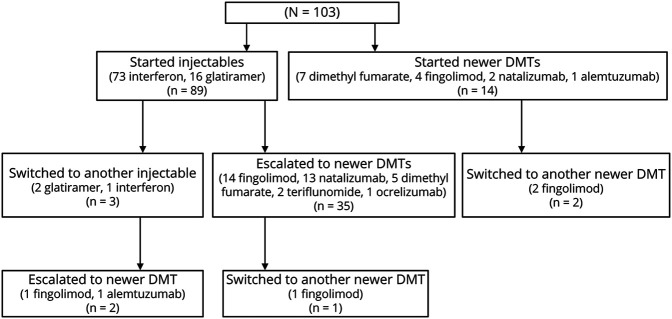
In this retrospective, multicenter study, from the UK Childhood Inflammatory Demyelination Network, we identified children with RRMS receiving DMTs from January 2012 to December 2018. Clinical and paraclinical data were retrieved from the medical records. Annualized relapse rates (ARRs) before and on treatment, time to relapse, time to new MRI lesions, and change in Expanded Disability Status Scale (EDSS) score were calculated.
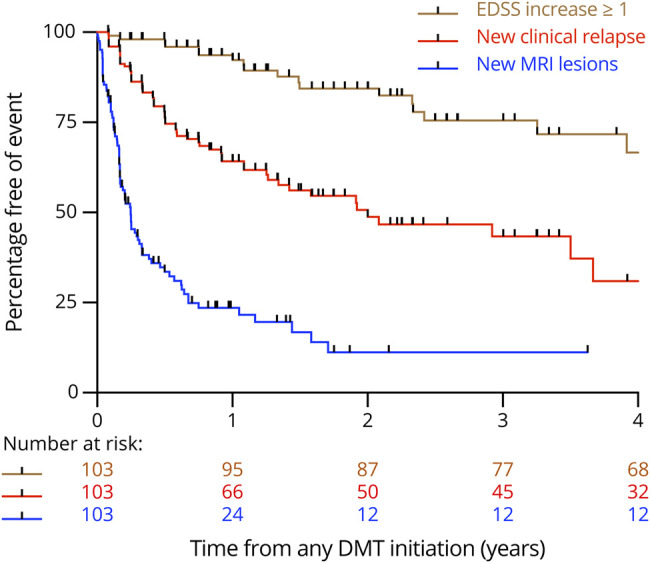
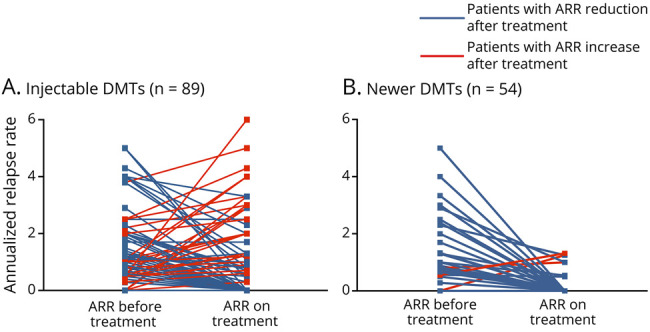
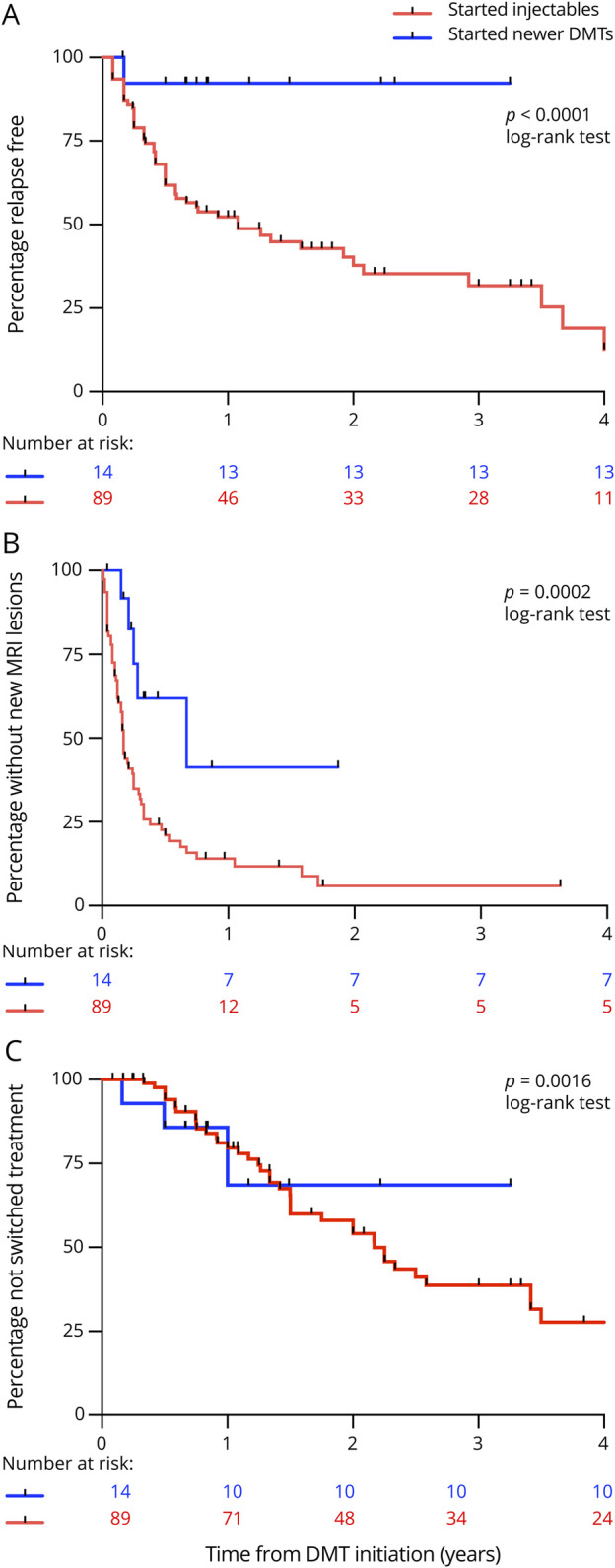
Of 103 children treated with DMTs, followed up for 3.8 years, relapses on treatment were recorded in 53/89 (59.5%) on injectables vs 8/54 (15%) on newer DMTs. The ARR was reduced from 1.9 to 1.1 on injectables ( < 0.001) vs 1.6 to 0.3 on newer DMTs ( = 0.002). New MRI lesions occurred in 77/89 (86.5%) of patients on injectables vs 26/54 (47%) on newer DMTs ( = 0.0001). Children on newer DMTs showed longer time to relapse, time to switch treatment, and time to new radiologic activity than patients on injectables (log-rank < 0.01). After adjustment for potential confounders, multivariable analysis showed that injectables were associated with 12-fold increased risk of clinical relapse (adjusted hazard ratio [HR] = 12.12, 95% CI = 1.64-89.87, = 0.015) and a 2-fold increased risk of new radiologic activity (adjusted HR = 2.78, 95% CI = 1.08-7.13, = 0.034) compared with newer DMTs. At 2 years from treatment initiation, 38/103 (37%) patients had MRI activity in the absence of clinical relapses. The EDSS score did not change during the follow-up, and only 2 patients had cognitive impairment.
Newer DMTs were associated with a lower risk of clinical and radiologic relapses in patients compared with injectables. Our study adds weight to the argument for an imminent shift in practice toward the use of newer, more efficacious DMTs in the first instance.
This study provides Class IV evidence that newer DMTs (oral or infusions) are superior to injectables (interferon beta/glatiramer acetate) in reducing both clinical relapses and radiologic activity in children with RRMS.
比较新型疾病修正疗法(DMT)与注射剂在复发缓解型多发性硬化症(RRMS)患儿中的真实世界疗效。
在这项来自英国儿童炎症性脱髓鞘网络的回顾性多中心研究中,我们纳入了 2012 年 1 月至 2018 年 12 月期间接受 DMT 治疗的 RRMS 患儿。从病历中提取临床和辅助检查数据。计算治疗前和治疗期间的年化复发率(ARR)、复发时间、新 MRI 病变时间和扩展残疾状态量表(EDSS)评分变化。
在 103 名接受 DMT 治疗的患儿中,89 名患儿(96.4%)完成了 3.8 年的随访,89 名患儿中有 53 名(59.5%)在接受注射剂治疗时有复发,54 名患儿中有 8 名(15%)在接受新型 DMT 时有复发。注射剂组的 ARR 从 1.9 降至 1.1(<0.001),新型 DMT 组从 1.6 降至 0.3(=0.002)。在 89 名接受注射剂治疗的患儿中,77 名(86.5%)有新的 MRI 病变,而在 54 名接受新型 DMT 治疗的患儿中,有 26 名(47%)有新的 MRI 病变(=0.0001)。新型 DMT 组患儿的复发时间、开始新治疗的时间和出现新影像学活动的时间均长于注射剂组(对数秩检验<0.01)。在调整了潜在混杂因素后,多变量分析显示,与新型 DMT 相比,注射剂与 12 倍的临床复发风险(校正后的危险比[HR]为 12.12,95%置信区间[CI]为 1.64-89.87,=0.015)和 2 倍的新影像学活动风险(校正后的 HR 为 2.78,95% CI 为 1.08-7.13,=0.034)相关。在治疗开始后 2 年,103 名患儿中有 38 名(37%)在无临床复发的情况下存在 MRI 活动。在随访期间 EDSS 评分没有变化,只有 2 名患儿有认知障碍。
与注射剂相比,新型 DMT 可降低 RRMS 患儿的临床和影像学复发风险。我们的研究为实践中即将向新型、更有效的 DMT 转变的观点提供了更多证据。
这项研究提供了 IV 级证据,表明新型 DMT(口服或输注)在降低 RRMS 患儿的临床和影像学复发方面优于注射剂(干扰素β/格拉替雷)。