Department of Pediatric Neurology, National Referral Center for Rare Inflammatory Brain and Spinal Diseases, Hopitaux Universitaires Paris-Sud, Le Kremlin-Bicetre, France
Immunology of Viral Infections and Autoimmune Diseases, Universite Paris 11 Faculte de Medecine, Le Kremlin-Bicetre, France.
J Neurol Neurosurg Psychiatry. 2020 Jan;91(1):58-66. doi: 10.1136/jnnp-2019-321124. Epub 2019 Aug 29.
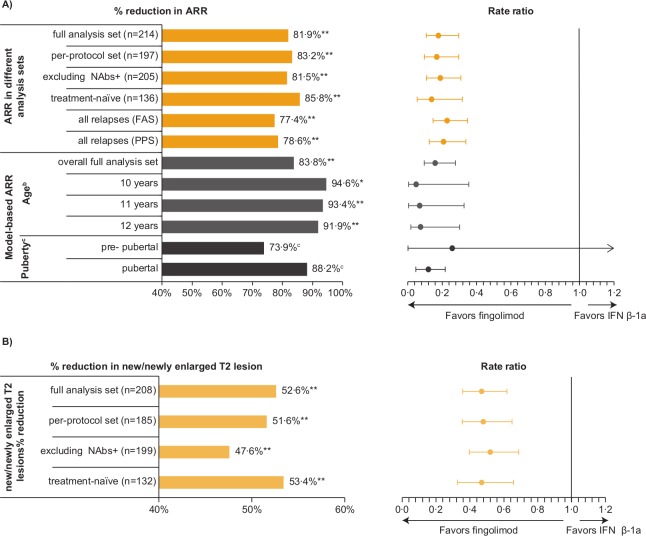
In PARADIG, a double-blind phase III trial in 215 paediatric patients with multiple sclerosis (MS) (10 to <18 years), fingolimod administered for up to 2 years significantly reduced the annualised relapse rate (ARR) and rate of new/newly enlarged T2 (n/neT2) lesions compared with interferon (IFN) β-1a.
To investigate (1) differences between treatment groups across subpopulations (treatment-naïve, younger/prepubertal patients); (2) disability progression.
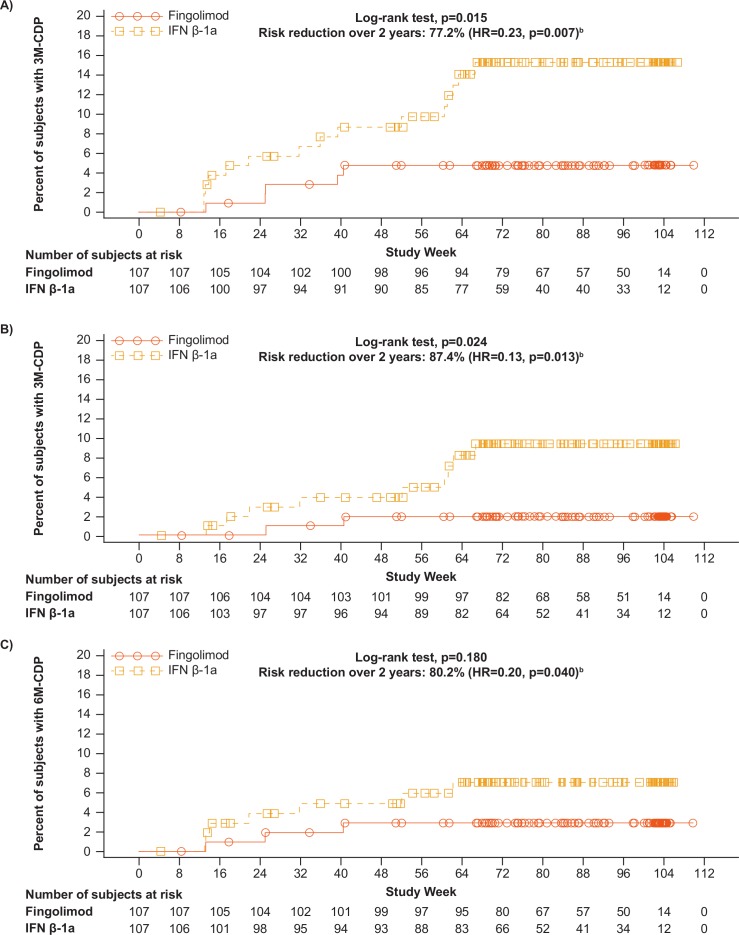
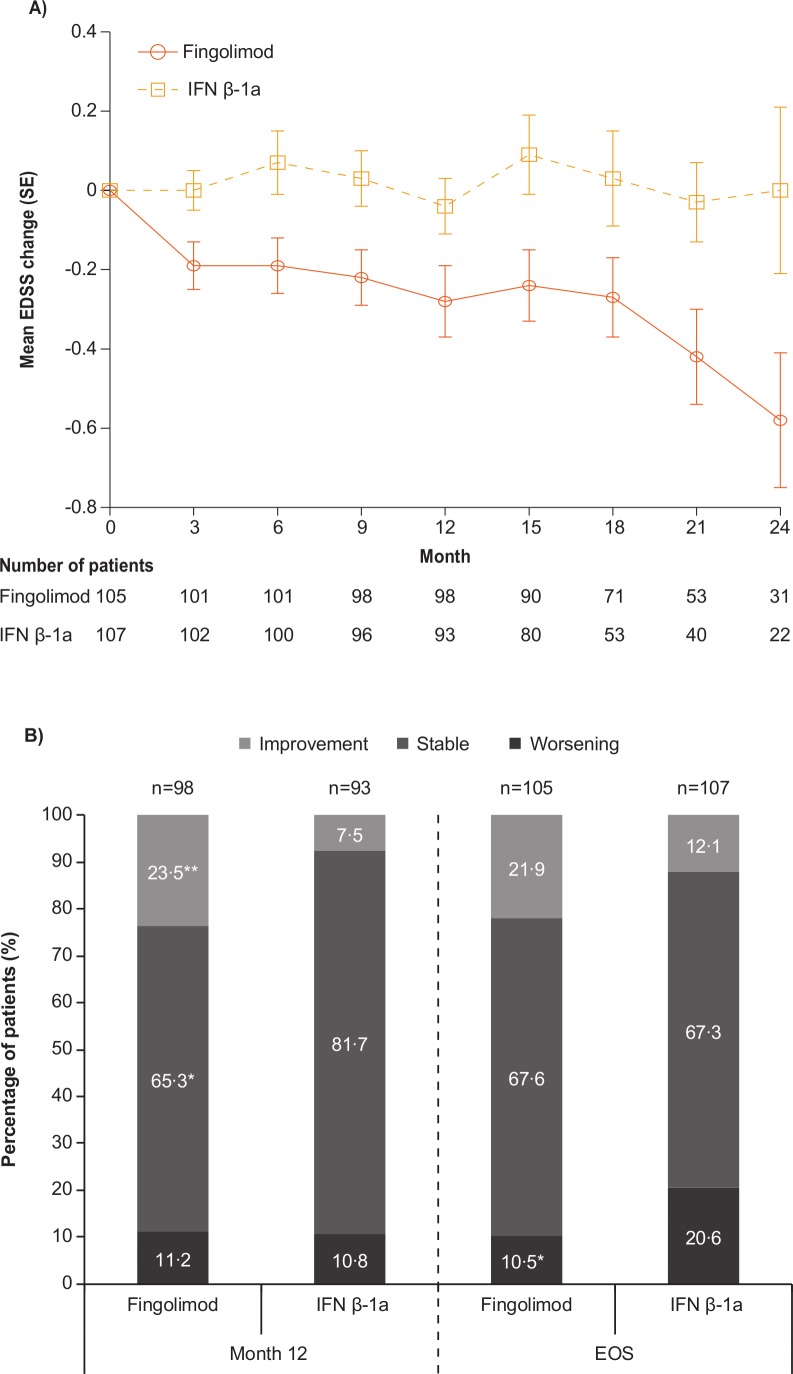
ARRs at 10, 11 and 12 years were estimated based on predefined modelling extrapolations. Changes in Expanded Disability Status Scale (EDSS), and in 3 month (3M) and 6 month (6M) confirmed disability progression (CDP) were evaluated post hoc.
In the treatment-naïve subpopulation, fingolimod reduced ARR and n/neT2 lesions by 85.8% and 53.4%, respectively versus INF β-1a (both p<0.001), compared with 81.9% and 52.6% in the overall population. Model-based ARR reductions in younger patients (≤12 years) were 91.9%-94.6%. Twice as many IFN β-1a-treated than fingolimod-treated patients had worse EDSS scores at study end (20.6% vs 10.5%, p=0.043). Risk reductions in 3M-CDP and 6M-CDP were 77.2% (p=0.007) and 80.2% (p=0.040), respectively.
Fingolimod in paediatric MS was associated with consistent control of disease activity versus IFN β-1a (including treatment-naïve and younger patients) and resulted in less disability progression for up to 2 years.
NCT01892722.
在 PARADIG 试验中,215 名多发性硬化症(MS)儿科患者(年龄为 10 至<18 岁)接受了为期 2 年的双盲 III 期临床试验,与干扰素(IFN)β-1a 相比, fingolimod 可显著降低年复发率(ARR)和新/新扩大 T2(n/neT2)病变的发生率。
研究(1)治疗组在亚组人群(初治患者、年轻/青春期前患者)中的差异;(2)残疾进展。
基于预设模型外推,估计 10、11 和 12 年的 ARR。事后评估扩展残疾状况量表(EDSS)以及 3 个月(3M)和 6 个月(6M)确认的残疾进展(CDP)的变化。
在初治亚组中,fingolimod 与 IFN β-1a 相比,ARR 和 n/neT2 病变分别降低了 85.8%和 53.4%(均 p<0.001),而总体人群中分别降低了 81.9%和 52.6%。年轻患者(≤12 岁)的模型预测 ARR 降低了 91.9%-94.6%。与 fingolimod 治疗组相比,接受 IFN β-1a 治疗的患者中,在研究结束时 EDSS 评分恶化的患者人数增加了一倍(20.6%比 10.5%,p=0.043)。3M-CDP 和 6M-CDP 的风险降低分别为 77.2%(p=0.007)和 80.2%(p=0.040)。
在儿科多发性硬化症患者中,fingolimod 与 IFN β-1a 相比可持续控制疾病活动(包括初治患者和年轻患者),并在长达 2 年内导致残疾进展减少。
NCT01892722。